 |
|
RECOMMENDED CONCISE
|
|
Statins, a critical review
|
|
|
|
| LDL, the blood transport for cholesterol & fats |
|
Pharma's myth and ignoring the
cause
1.
The
cholesterol myth.
Numerous critics have pointed out that cardiovascular disease is not
caused by higher levels of blood cholesterol or fats. Pharma promotes the cholesterol
myth and
ignores the major causes.
2.
Autopsy
studies of fatal MI found that fats and cholesterol are 7%-
22% of the atheroma.
3. Major
cause of cardiovascular disease is pathogens living within the middle layer of
artery walls. It initiates the immune
response which involves LDL and white blood cells.
4.
It
is in this immune function that the lipoprotein coating on LDL attaches to and
neutralizes certain toxins produced by pathogens.
5. Fructose
a reactive sugar is consumed at 8 times the paleo level. It damages the
mitochondria which supply the ATP molecule which supplies the
energy for over 90% of the reactions in the cells. Lowering it is
pathogenic. Excess fructose has made humans the sickest of mammals.
6. Carbon
monoxide mainly from tobacco and monosodium urate crystals damage the
endothelial cells that keep pathogens from entering the artery walls.
Fructose stimulates the production of uric acid, and statins lower the ATP
which keeps the endothelial cell properly functioning. 7.
LDL
is actively transported to the site of inflammation both to attach to toxins,
and because its contents of cholesterol and fats are needed as part of the
repair process, growing new cells.
8.
Statins,
carbon monoxide, and fructose are the main causes of cardiovascular
disease .
For confirmation from journal articles on primary role
of infective agent enter into http://scholar.google.com/ terms such as bacteria
+ atherosclerosis or go to http://healthfully.org/rl/id9.html for collection of articles
Statins a 6 Page Critical
Review 6/12/2022 http://healthfully.org/rc/id6.html
STATINS
Promotes cataracts diabetes, arterial and kidney disease, calcification,
insulin resistance, atherosclerosis, etc.
Okuyama, Harumi, Peter Langsjoen, et al May 2016, Medicines and
vegetables oils as hidden causes of cardiovascular disease and diabetes https://www.karger.com/Article/Pdf/446704 FULL
abbreviations: AD Alzheimer’s disease
AS Atherosclerosis ATP Adenosine triphosphate CHF
coronary heart failure CVD
cardiovascular disease LDL low density
lipoproteins TC total cholesterol
It is essential for you to understand
how pharma (pharmaceutical 0industry)
distorts,
controls medical information, and guidelines, thus the
practice of medicine--see Market Science and
Misinformation side effects. Marketing
pitch for the statins is based on high Total
Cholesterol (TC) and LDL causing
heart attacks, strokes and, Cardiovascular
Disease (CVD); but CVD is caused by bacterial and viruses
within the artery wall (tunica
media) and the immune system’s response, thus lowering cholesterol
doesn’t work--see
Cholesterol Myth.
LDL has 2 functions, one is to
as needed actively transport to cells cholesterol and triglycerides (fat), the
other is its immune-system function: it neutralizes (binds) toxins
produced by pathogens—see.
LDL in the artery walls is a sign of
pathogens causing inflammation. Thus,
the presences of LDL, cholesterol, and triglycerides in the plaque of artery
walls is because of LDL’s
immune function, and to promote the repair process,
since
triglycerides are essential components for cells and thus are needed for new
cells replacing infected ones and repair of damaged ones in the artery
wall. LDL is like a fireman and lumber
truck at a fire, a response to the pathogenic assault. Lowering LDL hinders
healing.
The doggy clinical trials ran for
marketing purposes fail to show significant reduction in deaths, so pharma
markets statins based on lowering cholesterol and rigs the clinical
guidelines.[1] Marketing and influence trumps medical
science. The best-selling
drug of all times is atorvastatin (Lipitor)
by Pfizer has US sales $12.4 billion in 2008, and world-wide total sales of
$131 billion by 2007, and that is one of 10 major statins on the market. With
50% of the men and 36% of the
women age 65 to 74 are taking statins (CDC/NCHS, Health, US, 2010); their
human costs are incredible: A) wasted
healthcare funds, B) misdirected research efforts and dietary choices, C) the
side effects are about 10-fold greater than the pharma-generated literature,
and this includes dementia, cognitive decline, lower ATP production, and heart
failure. Using pharma’s studies, it is
has been shown that women, those with congestive heart failure, and those above
the age of 70 do not benefit from statins –but they still get statins. The most profitable of all drugs
buries
alternatives that lower CVD[2] The cholesterol
myth sells drugs—watch YouTube
documentaries.
Statins discovery and approval casts doubts.
In the early 1970s an extract from a fungus
was shown reduce serum cholesterol, but the Japanese research stopped because
of animal
toxicity & cancer. Using a
similar extract Merck
in 1978 developed Mevacor (lovastatin). This “’Statin produced significant toxicity
at high doses in a variety of animal
species” (ibid 520). Animal studies
showed it caused cancer (given the
20-year latency in humans, a risk
confirmed). Merck tested low-dose
Mevacor for homozygous familial
hypercholesterolemia. The FDA gave
approval for this rare condition. Once
approved--as is the norm--the population base was expanded based on “marketing
science”. Because statins lower TC
30%, they were pushed as the only
effective treatment for CVD. But weak
epidemiological association of elevated TC with CVD doesn’t
demonstrate cause. With in-house studies Merck and the
manufacturers of the 9 me-too statins sold the world on “safe-and-effective”.
In Braunwald’s, Heart Disease, 8th
Ed. P 2286: “safe, effective, and well-tolerated pharmacologic agents that have
greatly expanded the therapeutic armamentarium available to the physician to
treat disorders of lipid metabolism.”
But in Braunwald’s, p 1085 table, 3
of 4 listed studies didn’t support effective. Merck’s JUPITER
Study, 2008, is used to push
primary prevention, but has major internal inconsistency: the cooked results “do not support
primary
prevent of CVD”. Moreover,
“statin
therapy and top athletics seem to be almost incompatible,”73% dropped out.”
Statins
don’t extend life and their side
effects are grossly
under-reported. Because statins
don’t treat the causes of CVD,
they are ineffective; thus there is a chorus of marginalized critics.
Cognitive decline and dementia: ”This pilot study found an improvement in cognition with
discontinuation of statins … Statins may adversely affect cognition in patients
with dementia” a cross over study of patients with dementia found taking statin
cognitive -tested positive for AD, off statins no AD, back on statins AD, 2007. Type 2 diabetes is
now strongly associated with dementia however,
prior to statins a study found no cognitive decline with diabetes, the Framingham Heart Study.
“There is a clear reason why statins would promote Alzheimer's” 2009 seminal. The response by pharma is to fund dozens
of studies to prove that statins prevent dementia; however, it was never
approved by either guideline or the FDA to treat AD. Moreover, cholesterol has
a signaling
function in the brain (and elsewhere) where it controls clustering of lipids
and proteins. Lowering cholesterol hinders
cholesterol’s signalling functions. “The
cholesterol controls the clustering of amyloid precursor protein with gamma
secretase in GM1 lipid domains. Wiki
2022.
“Lowering CoQ10, causing mitochondrial dysfunction which is strongly
associated with AD; lowering ATP production reduces the rate of removal of beta
amyloid and tau proteins and Parkinson’s alpha synuclein,--all three protein have
misfolded a consequence of lowered ATP by statins.
Diabetes Statin
therapy impairs insulin sensitivity and insulin secretion based on clinical and
epidemiologic studies, increases risk up to 99% a metastudy found. The
mechanism is through blocking CoQ10, thereby lowering the metabolism of glucose
and increasing insulin resistance, which causes the large lipid droplets in the
beta cells which lower the production of insulin to cause diabetic
hyperglycosemia. Another found at 13 years for atorvastatin and rosuvastatin
was 439 cases per thousand at 13 years, 2013 BMJ. Profitable guidelines require statins which
increases
insulin resistance, increases diabetes comorbidities.
Major cause for atherosclerosis: the major cause a failure
of the systems which
prevent pathogens from entering arteries and the cause stresses. This has been
demonstrated before 1920 by
autopsy studies of plaque. Statins
because of its effects upon the mitochondrial rate of metabolism slow the
production of ATP, adenosine triphosphate, which provides the energy for
autophagy (repair systems) and immune systems among others, thereby causing
endothelia dysfunction, and every others system in the body. This allows the
pathogens to colonize in the
media tunica of the artery which can depending on type of pathogen, causes
atherosclerosis. They also hinder
hyperplasia and restenosis, weaken fibrous plaque, delay the replacement of
collagen, causes muscle changes, 2005,
etc.
Familial hypercholesterolemia isn’t associated with early death
or shorter lifespan, moreover, they
have a lower rate of cancer and infections, 2019
lectures, 16 min. Moreover, in a 35-page seminal article a
study of 1,000 patients, it found no
shorter lifespan or early death, before the era of statins, 1966. Guidelines treatment is high dose statins;
they die early from statins, not hypercholesteremia.
hypercholesterolemia, a
condition that isn’t: The only association of the lipid hypothesis
with CVD is in the lowest quality studies.
Like weapons of mass destruction in Iraq, the repetition creates belief,
and both are false. Of course,
experts had exposed that, but they
don’t have access to the media, give CME classes, write clinical guideline and
medical textbooks. Autopsy studies going
back to 1915 have found between 7 and 22% of lipids in the coronary artery that
leaked and caused the fatal MI. Analysis
of atheromas support the same. The
percentage of fibrogen increases and inflammation ends as it matures. Population
studies often involved fraud[3] The
Framingham Study found that those with the highest 20% cholesterol live the
longest. A summary of the shame is
covered by Adams’
2011. The message is getting out on the BBC and ABD
(Australia),
but it is burred by advertisements and pill pushers. The fat wing of that theory
fares the same: because
saturated fats don’t
become rancid while unsaturated
fat does--including in cell membranes.
The link to pathogens as to the
western high
fructose diet is well
established. The dietary
fix is verboten. How can the physicians
treat a condition that isn’t a condition, that isn’t associated with poor
health? They shouldn’t.
Epidemical and autopsy evidence:
Autopsy studies
comparing several countries,[4]
these studies have confirmed that those with low cholesterol have as much or
more atherosclerosis than those with high serum cholesterol. Confirming this
is for the US is that those
with the highest 20% cholesterol live longer than those with lower 80% (the
Framingham Study). Also confirming this
is a major study of those with an MI whose blood measurement of cholesterol was
taken in the hospital within 24 hours of the event. Also confirming is the angiograms
as to
vascular occlusion and the TC reading. For
those death from trauma, 123 cases “No relationship was present in any
age group. It is concluded that the incidence and severity of atherosclerosis in man is not directly correlated
with the blood serum cholesterol content.”[5] A list of other countries with
the same
findings, 6 articles in Prof. Uffe Ravnskov, Ignore the Awkward. P
44.
Inflammation
cytokine inflammation is caused by signaling in response to foreign substances
including pathogens, and foreign objects such as a splinter. “During an inflammatory response
cholesterol is loaded into immune cells including macrophages. The cholesterol
is a signal that activates
cytokine production and other inflammatory
responses.“ To hinder the
healthful signaling response entails a worse prognosis.
[1] New guidelines (3/2014) based on a 10-year 7.5% risk for MI
would put 87% of men and & 56% of women age 60-75 on statins. These pharma
friendly guidelines exaggerate
the risk of MI 175% and expand statins use to nearly all men over 50 years.
[2] See
the 8-page paper ”On Lifestyle Diet and Drugs, or 2-page summation”. Two
studies have shown using raw
data
that positive bias is 32%.for pharma’s clinical trials. Pharma’s business model
drives them to marketing patented drugs for chronic conditions, most of which
are ineffective.
[3] Ben Goldacre Bad
Pharma (2012) goes into the many of those ways.
[4] Patterson, JC, Rosemary
Armstrong, et al, Feb 1962 Serum lipid levels and the severity of coronary
and cerebral atherosclerosis in adequately nourished men, 60 to 69 years of
age FULL An autopsy
study “failing to show any impressive
relationship between the serum lipid levels and the severity of disease” at
P 229 Hospitals were in London,
Canada, “We conclude from these results that the validity of the ‘lipid theory’
of atherosclerosis remains unproved, as far as the coronary arteries are
concerned.”
36 NEGATIVE EFFECTS: One, Erectile dysfunction, it lowers testosterone ,
and nitrous oxide
thus causes erectile dysfunction (ED);
a similar effect upon women for the steroids are synthesized from cholesterol. Since
both estradiol
and testosterone
are essential for optimal health, the lower of both promotes much more than the
ischemic events they are taken to prevent.
Two, COX-2
inhibitor, just like Vioxx, which increased heart attacks (MIs) over 300%[1]. The American Heart Association warns: “accumulated evidence that
non-steroidal, anti-inflammatory drugs [COX inhibitors], with the exception of aspirin;
they increase the risks
for heart attack and stroke”--promote
atherogenesis. Three, blocks production of
Q10, which enters LDL and
inhibits oxidative
damage that causes atherogenesis, and. Four, Plaque instability: “Vulnerability of plaques to
rupture and thrombosis is of greater clinical relevance than
the degree of stenosis they cause” (Corti et
al., 2003).
“Statins affect plaque stability in a variety of ways. The meta-lop-proteinases degrade extra-cellular
matrix components and thus “weaken the fibrous cap and destabilize the
lesions” -- Goodman and Gilman pharmacology, 11th Ed, p
950. Rupture of plaque causes over
80% of MIs. Statins
inhibit secretion MMP-1, 3, & 9 from SMC, and microphages
make plaque less stable. Five,
reduction in
ATP: Q10 is needed for the conversion
of APD to ATP
(adenosine-5-triphosphate), the source of energy for muscles contraction. “ATP is often called the ‘molecular unit of currency’
of intracellular energy transfer including
muscle contraction and for chemical reactions. ATP transports chemical energy within cells for metabolism”--Wikipedia. “ATP is essential for normal heart muscle
function, metabolism of cellular components and other activities in cell life.”
reduction of 40% in CoQ10 is
accepted.[2] Six, The heart muscle
under stress needs more
ATP, not less.
This is why pharma excludes the elderly and
those with coronary heart failure (CHF)
from trials. Thus, “the
mean
age of ME/CFS patients dying from CHF [coronary
heart failure] are 2.5 years younger than the control group.” CHF
death rate
has tripled since 1989. In a review
of statins on depletion of Q10 concludes: “As the potency of statin drugs increases and
as the target LDL cholesterol level decreases, the severity of Q10 depletion
increases and heart-muscle function declines. This tragic scenario may very well
be prevented by using supplemental
Q10 with all HMG CoA reductase inhibitors [statins]” and,
and. Thus “Lower
cholesterol, poorer outcome in CHF
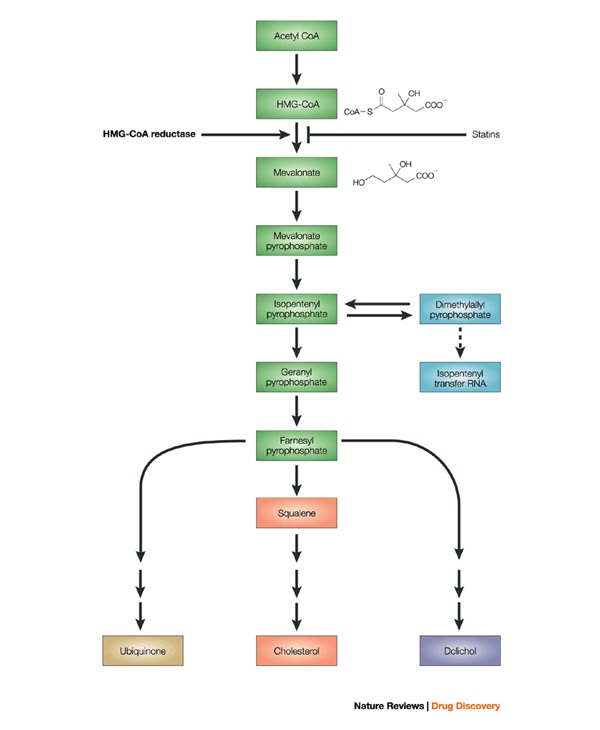
patients.” Pharma ignores Q10 side effect. Seven, All Statins inhibit the
rate controlling enzyme HMGCR of the
mevalonate pathway. “This pathway generates a range of other products in addition to cholesterol,
including
coenzyme Q10, heme-A, [dolichol], the production of dimethylallyl pyrophosphate (DMAP), & isopentenyl pyrophosphate (IPP), which serve as the
basis for the biosynthesis of molecules used in processes as diverse as terpenoid synthesis, protein prenylation and isoprenylated proteins which
have pivotal roles in cell biology and human physiology and potential relevance
to benefits as well as risks of statins. Drugs, such as the statins, stop the production of mevalonate by inhibiting HMG-CoA reductase” Wiki. “The
Mevalonate pathway is important for, cell membrane
maintenance, hormones, protein anchoring, and N-glycosylation. It is also a part of steroid biosynthesis” Wiki. “Dolichols are isoprenoids synthesized from mevalonate. They are vital to the
process of Glycoprotein formation in the endoplasmic
reticulum of cells. In this capacity
it is critical to the formation of the Glycoproteins involved in neuro-peptides, cell identification, cell messaging and Immune defense. Reduced bioavailability of dolichols can affect every cellular process in the body”
Wiki. And this
is only a partial list. Eight, Cholesterol is essential
for life. “It is the
precursor for the biosynthesis of
steroid hormones, bile acids,
vitamin D, and is an essential component of cell membranes for proper permeability. Effects include pancreatic
and hepatic dysfunction, ED, diabetes[3],
muscle weakness and myopathy
(muscle disease).
The myelin
is a cholesterol base coating around nerve cells[4]” (Wiki). Nine, Cognitive, the reduction Q10 & cholesterol for
the myelin sheath causes cognitive decline--especially in the elderly where it often leads to an incorrect
diagnosis of Alzheimer’s disease (AD)and
of neuropathy. Ten, Causes
Parkinson’s and Alzheimer’s diseases. These conditions are associated with low
level of cholesterol—at
Uffe p
56. In addition, I view
the accumulation of amyloid and tau proteins, which are toxic to the brain and
found in excess in all AD patients
is a result of lowered brain metabolism that diminishes the rate of the removal
of those proteins. Lower ATP thus is
causative of AD. Eleven Causes cancer a
confirmation of earlier animal studies—summary
of cancers, 25%
increase and. Twelve Stimulates atherosclerosis and heart disease
by blocking the vital CoQ10, heme
A, vitamin
K2 (the cofactor
for matrix Gla-protein activation) and biosynthesis of selenium containing
proteins, one of which is vital glutathione
peroxidase—at
2015. This
article states that “statins stimulate atherosclerosis and heart failure”, and
then provides the mechanisms. Thirteen Causes Interstitial
lung disease is similar to
emphysema in that it is a progressive condition that affects alveolar
epithelium and other tissues. Of FDA
reported side effects, it is 1/40th.
Fourteen, at ten years statins
doubles the rate in
women, at. Fifteen, diabetes is 46% more common, a 5.9 year study
found at Diabetes
doubles to triples the mortality rate. The number for senior must be at least
twice
that given their prevalence of insulin resistance for which type-2 diabetes in
an advance from of (see work of Dr. Joseph Kraft). See appendix for how statins
cause diabetes. Women ae at much higher rate on statins. Sixteen Polyneuropathy, damage
affecting peripheral nerves, features weakness, numbness, pain, etc. is 26
times more common after 2 years on statins compared to general matched population—at. Seventeen
Side effects
account for the poor
compliance in the elderly (75% stop within 2 years). Poor compliance also occurs
with elite athletes (see 1st pg.). Eighteen “Statins inhibit the
synthesis of vitamin K2, the cofactor for matrix Gla-protein
activation, which in turn protects arteries from calcification.” This
accumulation of calcium is causal for
atherosclerosis—one test for AS is the calcium score. Nineteen “Statins inhibit the
biosynthesis of selenium containing proteins, one of which is glutathione
peroxidase serving to suppress peroxidative stress” at 2015. The
reduction in glutathione entails increased oxidative damage,
thus statins are causal for all the conditions associated with oxidative
stress—quite a long list, see RAGE & diseases.
Twenty “An impairment of
selenoprotein biosynthesis may be a factor in congestive heart failure, reminiscent
of the dilated
cardiomyopathies seen with selenium deficiency” at 2015. Twenty one “Statins inhibit the synthesis of
vitamin K2, the
cofactor for matrix Gla-protein activation, which in turn protects arteries from calcification.” Calcification is the major causes of the
stiffness of arteries in atherosclerosis. This article by 7 Japanese professors
is titled Statins stimulate atherosclerosis
and heart failure: pharmacological mechanisms. Twenty-two, reduced production of heme A. In the important
respiratory protein cytochrome c oxidase, heme A plays an important role in the
oxygen center. Lowering heme, A
production through the melavonate pathway has many adverse effects. Twenty-three Adversely effects the
mitochondria by lowering the level of CoQ10 which among its other functions
acts as an antioxidant protecting the membrane and mtDNA. Twenty-four Statin administration
cause deficiency in selenium which
is causal for myopathy. Twenty-five treating the wrong cause, cholesterol, entails failure to research
for and develop effective treatments for CVD.
The major causes have, pathogens
in the artery walls; thus statins are ineffective. Three
out
of 4 major studies of secondary
prevention (ALL-HAT, ASCOT, & PROSPER) failed
to find life extension from statins (Table 42-78, Braunwald’s Supra,
p 1085). This
consistent failure even though scientific fraud (politely called Positive bias) is their business norm.
Such
negative results explain why pharma uses surrogate endpoint of lower
cholesterol instead of lives saved. This
table stands in opposition to the “safe
& effective” claim (p 2286),
which is pharma’s mantra, a mantra supported by their marketing studies and
guidelines. Junk science is the norm (p 3) on
TNT trial. Twenty-six
Primary prevention of high
risk patient is of no benefit huge meta-study found, in JAMA. Twenty-seven
fails to extend life of those with familial hypercholesterolemia
(those with extremely high cholesterol)[5]
at. Twenty-eight Liver functions are worse
and a few cases of liver failure (rhabdomyolysis), at. Twenty-nine, with long-term usage study (8.4 years) a 30%
increase in acute
kidney injury at Feb
2016. Thirty, drug
interaction with serious side effects are common, considering that over half of
senior in their 6th decade have taken statins, and seniors average
age 72 average 6 drugs according to a hospital emergency admission study (polypharmacy);
36
drug interactions. Thirty-one, both
low-fat diet and statin drug treatment increase susceptibility to Alzheimer’s,”
2009 seminal. To this I hold that the
reduced production of ATP results in a reduced rate of removal of tau protein,
beta amyloid, and misfolded alpha synuclein which is causal for Lewy body
dementia and Parkinson’s disease. Thirty-two, statins in blocking HMG-CoA
by 40% reduce the production of beta hydroxybutyrate by that amount, a brain
derived neurotropic factor (BDNF), and thus blocks a major compound which
promote a healthy brain. HMG-CoA is
converted to BDNF
in 2 steps.
Statins thereby promote dementia.
Thirty-three, dose increasing side
effects are the norm. A study of 50
consecutive heart patients taken off statin and given CoQ10, the report on
initial visit: (fatigue 84% to 12% at
one year, myalgia 64% to 6%, dyspnea 58% to 12%, memory loss 8% to 4%, Swedish
journal, 05. Thirty-four weight gain: Since statins through the lower of CoQ10 lowers
the product of the
energy molecule ATP it must lower the rate of metabolism and if all others
things don’t change (such as appetite reduction from nausea) then statins must
promote sedentary lifestyle through reduced rate of metabolism. Thirty-five, Cumulative effect: many of
the effects are a result of promotion of mitochondrial dysfunction and lower
CoQ10, which cause a lower production of ATP; this causes the large variety of
side effects known as conditions
associated with the western diet (CAWD)
which is driven by the lower production of ATP.
Thus, all of the long list of conditions of CAWD
are increased by use of a statin. Thirty six,
Anti-inflammatory effect: is a response to a positive-healing process,
therefore reducing the response increase the virulence of pathogenic causes and
slows the repair processes. Lowering
inflammation compromises the immune system.
For this reason statins effect upon prostaglandins statins like the
NSAIDs doesn’t inhibit atherogenesis, an inflammatory
process—see Vioxx, and.
[1]
A
reasonable assessment of total early deaths from the selective COX-2 inhibitors
in the US would be over 200,000; and a much greater number for the
non-selective COX inhibitors, the NSAIDs—but for aspirin. Celebrex is
still on the market, and though
warnings about all COX inhibitors
warning that they promote CVD, the
oft-heard sales message prevails.
[2]
After
3 months treatment of healthy patients with a poor TC using pravastatin
or simvastatin, the total
cholesterol and CoQ10
(Q10) were lowered 40%, when
compared to the placebo group. “A
diminution of Q10 availability may be the cause of membrane alteration with
consequent cellular
damage”—Journal of clinical Pharmacology. This finding is supported in other studies
and widely accepted—summary article.
[3] In a cohort
study a 63% increased incidence of diabetes, NEJN
2015 also. The WHI
trial found a 48% increase for women, see.
[4] The 2nd
cause for neuropathy, the first low Q10.
The two are additive.
[5] In the study the
average cholesterol level was 331 (norm is below 200). Our studies provide no evidence that familial
hypercholesterolemia appreciably shortens life of affected individual, ether
male or female. On the contrary, they
show that high level of serum cholesterol are clearly compatible with survival
into the seventh and eight decades.
36 NEGATIVE
EFFECTS: One, Erectile dysfunction, it lowers testosterone , and
nitrous oxide thus causes erectile dysfunction (ED); a similar effect upon women for
the steroids are synthesized from cholesterol. Since both estradiol and testosterone are essential for optimal health,
the lower of both promotes much more than the ischemic events they are taken to
prevent. Two,
COX-2 inhibitor, just like Vioxx, which increased heart attacks (MIs) over 300%[1]. The American Heart Association warns: “accumulated evidence that non-steroidal, anti-inflammatory drugs [COX
inhibitors], with the exception of
aspirin; they increase the
risks for heart attack and stroke”--promote
atherogenesis. Three, blocks production
of
Q10, which enters LDL and inhibits oxidative
damage that
causes atherogenesis, and.
Four, Plaque instability: “Vulnerability of
plaques
to rupture and thrombosis is of greater clinical
relevance than
the degree of
stenosis they cause”
(Corti
et al., 2003). “Statins affect
plaque stability in a
variety of ways. The meta-lop-proteinases
degrade extra-cellular matrix components
and thus “weaken the fibrous cap and
destabilize the lesions” -- Goodman and Gilman pharmacology, 11th
Ed, p 950. Rupture of plaque causes
over 80% of MIs. Statins
inhibit
secretion MMP-1, 3, & 9 from SMC, and microphages make plaque less
stable. Five, reduction in ATP: Q10 is needed for the conversion of APD
to
ATP (adenosine-5-triphosphate), the source of energy for muscles
contraction. “ATP is often called the ‘molecular unit of currency’ of intracellular energy transfer including muscle
contraction and for chemical reactions. ATP
transports chemical energy within cells
for metabolism”--Wikipedia.
“ATP is essential for normal heart muscle function, metabolism of
cellular components and other activities in cell life.” reduction of 40% in CoQ10 is accepted.[2] Six, The heart muscle under stress needs more
ATP, not less.
This is why pharma excludes the elderly and those with coronary heart
failure (CHF) from trials. Thus, “the mean age of ME/CFS patients dying from CHF [coronary heart failure] are 2.5 years younger
than the control group.” CHF
death rate
has tripled since
1989. In a review
of statins on depletion of Q10 concludes:
“As the potency of statin drugs increases and
as the target LDL cholesterol level decreases, the severity of Q10 depletion
increases and heart-muscle function declines. This tragic scenario may very well
be prevented by using supplemental
Q10 with all HMG CoA reductase inhibitors [statins]” and, and. Thus “Lower
cholesterol,
poorer outcome in CHF patients.” Pharma ignores Q10 side effect. Seven,
All
Statins inhibit the rate controlling enzyme HMGCR of the mevalonate
pathway. “This pathway generates a range of other products in addition to
cholesterol, including coenzyme Q10, heme-A, [dolichol], the
production of dimethylallyl pyrophosphate (DMAP), & isopentenyl pyrophosphate (IPP), which serve as the basis for the biosynthesis of
molecules used in processes as diverse
as terpenoid synthesis, protein prenylation and
isoprenylated proteins which
have pivotal roles in cell biology and human physiology and potential relevance
to benefits as well as risks of statins. Drugs, such as the statins, stop the production of mevalonate by
inhibiting HMG-CoA reductase” Wiki. “The Mevalonate
pathway is important
for, cell
membrane maintenance, hormones, protein anchoring, and N-glycosylation. It is also a part of steroid biosynthesis” Wiki. “Dolichols are isoprenoids synthesized from mevalonate. They are vital to the process of Glycoprotein formation in the endoplasmic
reticulum of
cells. In this capacity it is critical to the formation of the Glycoproteins involved in neuro-peptides, cell identification, cell messaging and Immune defense. Reduced bioavailability of dolichols can affect every cellular process in the body” Wiki. And this is only a
partial list. Eight, Cholesterol is essential for life.
“It is the precursor for
the biosynthesis of steroid
hormones, bile acids, vitamin D, and
is an essential component of cell
membranes for proper permeability. Effects include pancreatic and hepatic dysfunction, ED, diabetes[3],
muscle weakness and myopathy (muscle
disease). The
myelin
is a cholesterol base coating around nerve cells[4]”
(Wiki).
Nine,
Cognitive, the reduction Q10 &
cholesterol for the myelin sheath
causes cognitive decline--especially in the elderly where it often leads to an incorrect diagnosis of Alzheimer’s
disease (AD)and of neuropathy. Ten, Causes Parkinson’s and Alzheimer’s diseases. These conditions are associated with low
level of cholesterol—at
Uffe p 56. In addition, I view
the accumulation of amyloid and tau proteins, which are toxic to the brain and
found in excess in all AD patients
is a result of lowered brain metabolism that diminishes the rate of the removal
of those proteins. Lower ATP thus is
causative of AD. Eleven Causes cancer a
confirmation of earlier animal studies—summary
of cancers, 25%
increase and. Twelve Stimulates
atherosclerosis and heart disease
by blocking the vital CoQ10, heme
A, vitamin
K2 (the cofactor for
matrix Gla-protein activation) and
biosynthesis of selenium containing proteins, one of which is vital glutathione
peroxidase—at
2015. This article states
that “statins stimulate atherosclerosis and heart failure”, and then provides
the mechanisms. Thirteen Causes Interstitial
lung disease is similar to emphysema
in
that it is a progressive condition that affects alveolar epithelium and other
tissues. Of FDA reported side effects,
it is 1/40th. Fourteen,
at
ten years statins doubles
the rate in
women, at. Fifteen, diabetes
is 46% more common, a 5.9 year study
found at Diabetes doubles to
triples the mortality rate. The number
for senior must be at least twice that given their prevalence of insulin
resistance for which type-2 diabetes in an advance from of (see work of Dr.
Joseph Kraft). See appendix for how
statins cause diabetes. Women ae at much
higher rate on statins. Sixteen Polyneuropathy, damage affecting
peripheral nerves, features weakness,
numbness, pain, etc. is 26 times more common after 2 years on statins compared
to general matched population—at. Seventeen Side effects account for the
poor
compliance in the elderly (75% stop within 2 years).
Poor
compliance also occurs with elite athletes (see 1st pg.). Eighteen “Statins inhibit the synthesis of
vitamin K2, the cofactor for matrix Gla-protein activation, which in
turn protects arteries from calcification.”
This accumulation of calcium is causal for atherosclerosis—one test for
AS is the calcium score. Nineteen “Statins
inhibit the biosynthesis of selenium containing proteins, one of which is
glutathione peroxidase serving to suppress peroxidative stress” at 2015. The reduction in glutathione
entails
increased oxidative damage, thus statins are causal for all the conditions
associated with oxidative stress—quite a long list, see RAGE & diseases.
Twenty “An impairment of selenoprotein biosynthesis may be a factor in
congestive heart failure, reminiscent of
the dilated cardiomyopathies seen with selenium deficiency” at 2015.
Twenty one “Statins inhibit the synthesis
of vitamin K2,
the cofactor for matrix Gla-protein activation, which in turn protects arteries from calcification.” Calcification is the major causes of the
stiffness of arteries in atherosclerosis. This article by 7 Japanese professors
is titled Statins stimulate atherosclerosis
and heart failure: pharmacological mechanisms. Twenty-two, reduced
production of heme A. In the
important
respiratory protein cytochrome c oxidase, heme A plays an important role in the
oxygen center. Lowering heme, A
production through the melavonate pathway has many adverse effects. Twenty-three Adversely effects the mitochondria
by lowering the level of CoQ10 which among its other functions acts as an
antioxidant protecting the membrane and mtDNA.
Twenty-four Statin administration cause deficiency
in selenium which is causal for myopathy. Twenty-five treating the wrong cause,
cholesterol, entails failure to research for and develop effective treatments
for CVD.
The major causes have, pathogens
in the artery walls;
thus statins are ineffective.
Three
out of 4 major studies of secondary
prevention (ALL-HAT, ASCOT, & PROSPER) failed
to find life extension from statins (Table 42-78, Braunwald’s Supra,
p 1085). This
consistent failure even though scientific fraud (politely called Positive bias) is their business norm. Such negative results explain why
pharma uses
surrogate endpoint of lower cholesterol instead of lives saved. This table stands
in opposition to the “safe & effective”
claim (p 2286), which is pharma’s mantra, a mantra
supported by their marketing studies and guidelines. Junk science is the norm
(p 3) on
TNT trial.
Twenty-six Primary prevention
of high risk patient is of no benefit huge meta-study found, in JAMA.
Twenty-seven fails to extend life
of those with
familial hypercholesterolemia (those with extremely high cholesterol)[5] at. Twenty-eight Liver
functions are worse and a few cases of liver failure (rhabdomyolysis), at. Twenty-nine, with
long-term usage study (8.4 years) a 30% increase in acute kidney injury at Feb
2016.
Thirty, drug interaction with serious side effects
are common, considering that over half of senior in their 6th decade
have taken statins, and seniors average age 72 average 6 drugs according to a
hospital emergency admission study (polypharmacy); 36
drug interactions.
Thirty-one,
both
low-fat diet and statin drug treatment increase susceptibility to Alzheimer’s,”
2009 seminal. To
this I hold that the reduced production of
ATP results in a reduced rate of removal of tau protein, beta amyloid, and misfolded
alpha synuclein which is causal for Lewy body dementia and Parkinson’s
disease. Cholesterol is a signal molecule
which prevents the clustering of lipids, that function is compromised by
statins. Thirty-two, statins in blocking HMG-CoA by 40%
reduce the production of beta hydroxybutyrate by that amount, a brain derived
neurotropic factor (BDNF), and thus blocks a major compound which promote a
healthy brain. HMG-CoA is converted to BDNF
in 2 steps.
Statins thereby
promote dementia. Thirty-three, dose increasing side effects are the norm.
A study of 50 consecutive heart patients
taken off statin and given CoQ10, the report on initial visit: (fatigue 84%
to 12% at one year, myalgia 64%
to 6%, dyspnea 58% to 12%, memory loss 8% to 4%, Swedish
journal, 05.
Thirty-four weight
gain: Since
statins through the lower of CoQ10 lowers the product of the energy molecule
ATP it must lower the rate of metabolism and if all others things don’t change
(such as appetite reduction from nausea) then statins must promote sedentary
lifestyle through reduced rate of metabolism.
Thirty-five,
Cumulative
effect: many of the effects are a result of promotion of mitochondrial
dysfunction and lower CoQ10, which cause a lower production of ATP; this causes
the large variety of side effects known as conditions
associated with the western diet (CAWD)
which is driven by the lower production of ATP.
Thus, all of the long
list of conditions of CAWD are increased by use
of a
statin. Thirty six, Anti-inflammatory effect: is a response to
a positive-healing process, therefore reducing the response increase the
virulence of pathogenic causes and slows the repair processes. Lowering inflammation
compromises the immune
system. For this reason statins effect
upon prostaglandins statins like the NSAIDs doesn’t inhibit atherogenesis, an inflammatory
process—see
Vioxx,
and.
One POSITIVE
EFFECTS: 12) Statins, like
aspirin, reduce
clotting and thus the risk for thrombosis.
Statins
“down-regulate transcriptional activities of NF-kappa B, AP-1, and HIF-1a with
coordinate reduction in expression of pro-thrombotic and inflammatory
cytokines” at
2006.
But rather than promote as an
anti-inflammatory drug, and thereby thus by extension aspirin, pharma pitches only
lowering total cholesterol.[6] Pharma is against
aspirin
because aspirin lowers significantly lowers the
risk for CVD, dementia, and cancer.
[1]
A
reasonable assessment of total early deaths from the selective COX-2 inhibitors
in the US would be over 200,000; and a much greater number for the
non-selective COX inhibitors, the NSAIDs—but for aspirin. Celebrex is
still on the market, and though
warnings about all COX inhibitors
warning that they promote CVD, the
oft-heard sales message prevails.
[2]
After
3 months treatment of healthy patients with a poor TC using pravastatin
or simvastatin, the total
cholesterol and CoQ10
(Q10) were lowered 40%, when
compared to the placebo group. “A
diminution of Q10 availability may be the cause of membrane alteration with
consequent cellular
damage”—Journal of clinical Pharmacology. This finding is supported in other studies
and widely accepted—summary article.
[3] In a cohort
study a 63% increased incidence of diabetes, NEJN
2015 also. The WHI
trial found a 48% increase for women, see.
[4] The 2nd
cause for neuropathy, the first low Q10.
The two are additive.
[5] In the study the
average cholesterol level was 331 (norm is below 200). Our studies provide no evidence that familial
hypercholesterolemia appreciably shortens life of affected individual, ether
male or female. On the contrary, they
show that high level of serum cholesterol are clearly compatible with survival
into the seventh and eight decades.
[6] A very important
distinction is that downregulating the inflammatory process is healthful only
for certain pathologies and high-risk situation such as an ischemic event from
underlying atherosclerosis. This benefit
occurs at the expense of reducing immune system functions and certain healing
processes. The inflammatory system is
there for a purpose, and in healthy people taking regularly an
anti-inflammatory drug do more harm,
than good. It is better to treat the primary cause than the secondary
effect.
|
|
|
| cholesterol synthesis, statin (HMG-CoA) blocks |
|
| vital synthesis of ubiquinoe (Q10), etc. |
On statins: Since
“cholesterol
synthesis occurs mostly at night” (Wiki). If you must lower TC it should
be done at night.
with short half-life[1]
support a slow-release pill or long acting: Zocor 2, Lipitor 14, Crestor
19 hours. niacin 35 min
Sorting
it out, RECOMMENDATIONS (for myself): Atherogenesis
is caused pathogens within the artery
walls.
This initiates an inflammatory immune
response by macrophages. LDL
which has an immune response is actively
transported into the artery walls where it contents cholesterol and
triglycerides form new and repair damaged cells. Because
of this transport process, lowering LDL doesn’t affect the formation of plaque,
thus statins don’t stop plaque formation (see illustration). The 32%
drop in deaths from heart attacks
and strokes (1960 to 1992) occurred prior to statins, the percentage of smokers
dropped from 46% to under 20%, and a pack a day increase the death rate from
heart attacks by over 100%. With
statins’ wide use, mortality rate has remained
constant. Mevacor was approved in 1987; only 60,000
taking it by 1990. Reduced death rate
was from a reduction in smoking that goes along with taking a heart-healthy
drug, and because of scientific fraud committed in industry funded
studies—studies are a marketing tool. Statins
reduce quality of life for the elderly: a large Canadian
study had 75% dropout by 2 years, and 80% in a
NJ
study. Very common and under
reported side effects are fatigue, muscle
weakness & cramps, mental confusion, pancreatic and liver dysfunction,
diabetes, indigestion, cognitive decline, erectile dysfunction, & lower libido,
especially for the elderly. Lowering TC
with statins doesn’t affect the young
unstable plaque that causes 95% MIs because pathogens are the cause
of the plaque formation. What to do: I wouldn’t
take a statin
because they do not reduce mortality;
they aren’t worth their side effects & expense. Lifestyle changes of low carbohydrate-sugar diet lowers damage to endothelial cells on the
artery walls. Damage is caused mainly by
glycation by fructose (a net 15 times the rate of glucose, 7.5 times more
reactive and in the cells at least twice as long because glucose is metabolized
first before fructose). Avoid carbon
monoxide (cigarettes main source) which exacerbates the damage. Endothelial
cells block the migration of
pathogens. Saturated and monounsaturated fats are the best source of
energy. Everyone should take the
antioxidants ascorbic acid and Q10, prevent oxidative
damage. Take 325 mg aspirin[2] uncoated daily to prevent
blood clots that forms when plaque leaks from a coronary artery thus lowering
ischemic events, etc5. Low
dose aspirin is ineffective because of tolerance after 1 year. Take the natural
estrogen (estradiol) &
progesterone at menopause. Estrogen[3] lowers risk of CVD 50%,
osteoporosis and much more. For elderly
men testosterone lowers risk & increases survival from
an MI. Pharma attacks hormones &
aspirin because they work. Read Marking Science, be skeptical of
medical “wisdom.” If you still want to
lower total cholesterol, then take 250 mg slow release niacin or inositol
hexanicotinate at night, when
it is effective. Insulin produced
following meals blocks the lipid lowering effect of niacin inositol &
statins. High dose during the day is a
pharma ploy to reduce the use of niacin.
JK has exercised
vigorously since 1975; takes
325 mg uncoated aspirin daily since 1992-2017 and started again in 2020; DHEA 30
mg sublingually since 2002 testosterone high dose since 2004; low-sugar low
carb diet 2014, 300 mg CoQ10, and vitamin C 2000 mg (as calcium ascorbate) since
2014. Intermittent fasting (skipping
breakfast) since 2015, high saturated fat diet since 2016. Results: JK is 78 (2021) with excellent muscle tone and
strength, no joint pain, blood pressure averages 125/75, BMI 23, and runs 50
miles a month or more. JK is happily
retired with a significant other, and is writing a book on why humans are the
sickest of mammals. JK lements the
amount of harm caused by the high sugar western diet, and has through the
website and occasional class taught how our diet makes us the sickest of
mammals.
Expanding the market: Statins are
claimed by industry funded studies and their dupes as lowering the risk for
dementia, as a treatment for
NAFLD (fatty liver disease). The latter
would add 100 million more users.
Statins following guidelines is given to diabetics adding a potential 90
million. Statins are recommended as part
of the treatment for Alzheimer’s disease, and is recommended for treating
children with hypercholesterolemia, and there are other prophylactic uses. We
are back in the snake-oil days with NIH
stamp of approval and mass marketing.
Pharma spends 4-times more on physicians than on the public; don’t blame
the pill poppers and pill pushers, for pharma has a hot sale’s pitch that
creates social patterns of behavior. Sell
the fluff and burry the evidence. Humans
are a social animal, marketing works.

The HMG-CoA
reductase pathway, which is blocked by statins via inhibiting the rate limiting
enzyme HMG-CoA
reductase. Reduces
the first compound in the chain, mevalonic acid an average 40%, thereby reduces
all subsequent products shown.
[1]
“Half-life (t½) the time that it takes
for the concentration in blood plasma of a substance to
reach one-half of its initial measured level “(Wiki).
[2] Aspirin
very
significant risk reduction of most major cancers and Alzheimer’s disease, plus it reduces mortality from
stage I,
II, III cancer
over
40%, and
by 4 mechanism atherogenesis.
The long-term risk
for
stomach bleeding is about 4%; comparable
to other NSAIDs and many other drugs. Pharma’s attack with FDAs help is
market driven. Low does not have an
anti-inflammatory effect and tolerance develops to its anti-platelet effect.
[3]
For
many
benefits of natural
HRT, and testosterone
for men;
and don’t
believe the marketing science about hormones.
^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^
TERMS: Primary prevention for those with high cholesterol
only. Secondary
prevention for those with pre-existing cardiovascular disease (CV). Opinion Leader: an authority in a specialty who receives substantial
income from pharma. Cardiovascular
Disease (CVD) any
disease, whether congenital or acquired, of the heart and blood vessels. Cholesterol
Profile (TC) the lab report listing the various components
of cholesterol. Coronary Heart
Disease (CHD) atherosclerotic
arterial deposits (atherosclerosis). Congestive
Heart Failure
(CHF)/ heart failure (HF)
occurs when the heart muscle is unable to maintain adequate circulation of
blood in the tissues of the body or to pump out the venous blood returned to it
by the venous circulation. Myocardial
Infraction (MI) a heart attack. HMG-CoA
reductase inhibitors (statins).
^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^
{more on it in word document}
Animal
studies are a very good indicator for potential side effects in humans: The original
studies are done on animals to find out if a drug is effective and safe. Unfortunately
when pharma funded they own the
results and as part of normal business do not published unfavorable
results. However, since such studies are
fairly inexpensive, a number of them of animal studies are part of graduate
work supervised by a professor, and are published. Others, like this review
are written by the
manufacturer, in this case Merck. The
article mentions the side effects and then concludes that they don’t occur in
“human therapeutic doses.” A large body
of evidence contradicts this rosy conclusion.
It is very disappointing that the top tier journal Nature published this
article, which is a sales pitch for Lipitor, dressed up as a review of the
research. (see the published summation below to dispel doubt) For example the
effects upon testosterone and
CoQ10 are not mentioned—though there is significant literature on their
suppression by Lipitor and other statins.
^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^
Below is an example of
marketing science. It is a review of the
research on Mevicor (Lovastatin) by Merck (hardly unbiased in their dismissal
of the relevance of animal studies).
Worth reading as to risk factors since animal studies have a high
carryover to humans. Tolbert left out
the “c” word cancer, for which this side effect in animals is be repeatedly
brought up. Since most cancers have a
20-year lag time (such as cigarettes) from exposure, short-term clinical trials
will not expose this risk. It took for
example 30 years for cancer to be associated with DES, a synthetic estrogen,
and 50 years for MPA (methoxyprogesterone, which is still on the market).
SIDE EFFECTS
ANIMALS: “Statins
produce significant
toxicity at high doses in a variety of animal species. These effects include
increases in hepatic transaminases, atypical focal hyperplasia of the liver,
squamous epithelial hyperplasia [ORGAN ENLARGEMENT] of the rat fore-stomach (an
organ not present in man), cataracts, vascular lesions in the central nervous
system (CNS), skeletal muscle toxicity, testicular degeneration and, although
the statins are clearly not genotoxic, tumours of the liver and other sites
(details can be found in the product circulars of the individual statins). It
has been shown, where it has been practical to conduct the experiment, that
these effects can be prevented by administering mevalonate 29,30, the product of the reaction
catalysed by HMG-CoA reductase. This
indicates that these toxic effects are mostly, if not entirely, attributable to
extreme inhibition of the enzyme at high doses 29. So
Merck, and the regulatory agencies considering
the marketing application submitted by Merck, were faced with a wide range of animal toxicological
effects, as well
as the history of compactin and the known central role of the cholesterol biosynthesis
pathway in many physiological processes, including the production of steroids
and cell membranes. [The structure Lovastin
is quite similar to compactin, whose toxicity in animal studies resulted from
it not being tested clinically; nevertheless Merck went forward.] Compactin
was withdrawn from the market for ] … Fortunately,
except for rare cases of myopathy and marked but asymptomatic increases in
hepatic transaminases, none of the adverse effects found in animals occur at
human therapeutic doses.” Nature Reviews
Drug Discovery 2, 517-526 (July 2003) | doi:10.1038/nrd1112. This Merck scientist is referring to
life-threatening and rare muscle destruction caused by statins. However, its
impact upon quality of life for
those above the age of 50 is gradual and thus subtle--the degree increases with
age.
Author’s affiliations: A. Tolbert,
Merck Research Laboratories,
Rahway, New Jersey 07065, USA.
Email: jonathan_tobert@merck.com
APPENDIX
How statins promote diabetes, by blocking malonyl-CoA, which is the
first step in converting the excess glucose into triglycerides. Extending the
excess glucose causes more
release of insulin and the turn on the PP producing furctose: The liver
starts actively making triglycerides from
excess glucose when it is supplied with glucose that cannot be oxidized or
stored as glycogen. This increases the concentration of malonyl-CoA, the first
intermediate in fatty acid synthesis, leading to the inhibition of carnitine
acyltransferase 1, thereby preventing fatty acid entry into the mitochondrial
matrix for β oxidation. This inhibition prevents fatty acid breakdown while
synthesis occurs. https://en.wikipedia.org/wiki/Carnitine#Regulation_of_fatty_acid_%CE%B2_oxidation
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Pharma's myth and ignoring the
cause
1.
The
cholesterol myth.
Numerous critics have pointed out that cardiovascular disease is not
caused by higher levels of blood cholesterol or fats. Pharma promotes the cholesterol
myth and
ignores the major causes.
2. Major cause of
cardiovascular disease is pathogens living within the middle layer of artery
walls. It initiates the immune response
which involves LDL, HDL, and white blood cells.
3. It is in this
immune function that the lipoprotein coating on LDL attaches to and neutralizes
certain toxins produced by pathogens.
4. Reactive
chemicals such as simple sugar fructose and carbon monoxide can potentiate
the process resulting in the formation of plaque within the artery walls by
damaging the endothelial cells lining the artery
walls thereby reducing the barrier of the endothelia cells to blood
borne pathogens.
5. LDL is actively
transported to the site of inflammation both to attach to toxins, and because
its contents of cholesterol and fats are needed as part of the repair
process..
For confirmation from journal articles on primary role of
infective agent enter into http://scholar.google.com/
terms such as bacteria + atherosclerosis or go to http://healthfully.org/rl/id9.html
for collection
of articles
For confirmation
of cholesterol myth enter into http://scholar.google.com/ or http://www.amazon.com/ cholesterol myth,
or go to http://healthfully.org/rl/id5.html
for collection of journal articles—for documentaries.
1. .
For confirmation from journal
articles on
primary role of infective agent enter into http://scholar.google.com/ terms such as bacteria +
atherosclerosis or go to http://healthfully.org/rl/id8.html for collection of articles.
For confirmation of cholesterol
myth enter into http://scholar.google.com/ or http://www.amazon.com/ cholesterol myth,
or go to http://healthfully.org/rl/id5.html for collection of
journal articles—for
documentaries.
Why is that much money being
wasted on a patented statin???
Last year, rosuvastatin (Crestor) was the most
prescribed brand name drug in the US, with 22.3 million prescriptions filled
and $5.8bn (£3.9bn; €5.5bn) in sales.1 Worldwide 2013
sales were $8.2bn, the third highest for any branded drug. Given the longstanding,
continuing evidence
of rosuvastatin’s comparative lack of clinical benefits and increasing evidence
of risks, how did this happen? The short answer is that of statins still on the
market, the milligram for milligram cholesterol lowering potency of
rosuvastatin exceeds all others, a fact exploited in advertising campaigns. But
what about actually improving health, preventing heart attacks and
strokes? http://www.bmj.com/content/350/bmj.h1388?etoc= Sidney Wolf, 3/17/15
Pfizer's Lipitor (atorvastatin),
which lost US
patent protection in 2011. as a result
of the settlement will now be able to sell its products on an exclusive basis
in the US between May 2 and July 8, 2016.
The substance patent for Crestor expires on January 8, 2016, but
AstraZeneca won a six-month extension under the US paediatric trials incentive
programme. http://www.pmlive.com/pharma_news/astrazeneca_settles_with_generic_rivals_in_crestor_patent_challenge_469203 
^^^^^^^^^^^^Non-technical summation
Statins and
cholesterol: Cardiovascular
disease (CVD) results from pathogens within the
artery walls that cause an inflammatory response by macrophages which results
in the formation of plaque. The risk of
infectious bacteria and viruses colonizing the artery walls is increased by artery
endothelial dysfunction (cells which line the artery walls and thereby control
the entry into the underlying tissue). Major causal factors for endothelial
dysfunction is a result of insulin resistance, and overstuffing cells with
glucose.. Insulin resistance is caused
by the high sugar (fructose) western diet.
Thus low carb
low sugar diet is the first line of prevention
and healing. Carbon
monoxide--main source smoking—can significantly exacerbate endothelial
dysfunction. Fructose and carbon monoxide
are reactive chemicals which damage the endothelial cells. A lower level of LDL doesn’t prevent the active transport
of LDL as part of the immune-healing response,
statins slow the healing process. A
large body of evidence has demonstrated that cholesterol and triglycerides are
mere bystanders, and that pathogen cause the inflammation resulting in
atherosclerosis. see
and watch documentaries.
Statins are the biggest scam in pharma’s history. And
it made all the worse not only by chasing
after causes which don’t protect against CVD, but also because of their affect
upon quality of life, which very significantly affect those above the age of
60.
Cholesterol is used to synthesize numerous essential compounds and is
part of cell membranes. Lowering its
production—typically 40%--has many side effects. Statins also lower the
production of CoQ10 by
40%. CoQ10 has an essential function in
the production of ATP, the body’s energy molecule. Statins for all these
reasons should not be
taken..
|
|
|
|
|
|
|
|
TERMS
Cardiovascular Disease (CVD) any disease, whether
congenital or
acquired, of the heart and blood vessels.
Cholesterol
Profile (CP) the amounts of High
density, low density, and very low density lipoproteins, of triglycerides, and
other blood borne compound that are indicators for angiogenesis.
Circulatory
failure occurs when in the blood
the concentration of oxygenated
hemoglobin in the arterial blood, or the vascular bed is responsible for the
inadequate cardiac output.
Congestive
Heart Failure (CHF) heart failure in which the
heart muscle is unable to maintain
adequate circulation of blood in the tissues of the body or to pump out the
venous blood returned to it by the venous circulation.
Coronary Failure (CF) heart failure in which the heart muscle
is
deprived of the blood necessary to meet its functional needs as a result of
narrowing or blocking of one or more of the coronary arteries.
Coronary Heart Disease (CHD) a disease of the heart and coronary
arteries that is characterized by atherosclerotic arterial deposits that block
blood flow to the heart, causing myocardial infraction.
Endotoxin, the toxic protoplasm liberated when a
microorganism dies and disintegrates.
Toxic substance bound to to the bacterial cell wall and releasedwhen the bacterium ruptures or disintegrates. Endotoxins consist
of lipopoly- saccharide and
lipoprotein complexes. The protein
component determines the antibody type that can react with the endotoxin
molecule to produce an immune reaction.
Endotoxins are rarely fatal, although they often cause fever.
Heart
Failure
(HF) is a pathophysiological state in which the heart is unable to
pump blood at a rate commensurate with the requirements of the metabolizing
tissues or can do so only from an elevated filling pressure. I t is usually, but not always caused by a
defect in myocardial contraction, i.e., by myocardial
failure
HMG-CoA reductase inhibitors
(statins), the enzyme they inhibit, which is the method by which lower cholesterol.
Meta-study
consists of grouping together studies according to a set of criteria and then
calculating the summation of finding.
Cochrane Library consists of hundreds of such meta-studies without
funding from PhARMA.
Morbidity
rate the relative incidence of a particular
disease in a specific locality
Myocardial
Infraction
(MI) heart attack
Primary
prevention for
those with high cholesterol, but no other health problems
Sarcopenia the loss of muscle mass causing weakness.
Statins contribute to this through lowering
of CoQ10, and thereby affecting exercise and physical exertion, which are
needed to maintain muscle mass and tone.
Secondary
prevention for those with pre-existing cardiovascular disease (CV) Sepsis, the poisoned condition resulting from the
presence of pathogens or their toxins.
The severe infection caused by pathogenic organisms, especially
bacteria, in the blood or tissues. If
untreated, a localized infection, as in the respiratory or urinary tracts, can
lead to infection in the blood stream and widespread inflammation,
characterized by fever, chills, and other symptoms and later septic shock. Chronic
infection is a causal factor for CVD.
Thought
Leader because of being PhARMA
friendly a few administrators and researchers
perform various well-paid services for PhARMA, such as a researcher, author of
textbooks, head of clinic, and giving educationals. They become known as an expert in their
specialty. ^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^
Below
is an example of marketing science. It
is a review of the research on Mevicor (Lovastatin) by Merck (hardly unbiased
in their dismissal of the relevance of animal studies). Worth reading as to
risk factors since animal
studies have a high carryover to humans.
Tolbert left out the “c” word
cancer, for which this side effect in animals is be repeatedly brought up. Since
most cancers have a 20-year lag time
(such as cigarettes) from exposure, short-term clinical trials will not expose
this risk. It took for example 30 years
for cancer to be associated with DES, a synthetic estrogen, and 50 years for
MPA (methoxyprogesterone, which is still on the market).
.
SIDE EFFECTS
ANIMALS: “Statins produce significant toxicity at high doses
in a variety of animal species. These effects include increases in hepatic
transaminases, atypical focal hyperplasia of the liver, squamous epithelial
hyperplasia [ORGAN ENLARGEMENT] of the rat fore-stomach (an organ not present
in man), cataracts, vascular lesions in the central nervous system (CNS), skeletal
muscle toxicity, testicular degeneration and, although the statins are clearly
not genotoxic, tumours of the liver and other sites (details can be found in
the product circulars of the individual statins). It has been shown, where it
has been practical to conduct the experiment, that these effects can be
prevented by administering mevalonate 29,30, the product of the reaction catalysed by HMG-CoA reductase. This indicates that these toxic effects are mostly,
if not entirely, attributable to extreme inhibition of the enzyme at high doses
29. So
Merck, and the regulatory agencies considering the marketing application
submitted by Merck, were faced with a wide range of
animal toxicological effects, as well as the history of compactin and
the known central role of the cholesterol biosynthesis pathway in many
physiological processes, including the production of steroids and cell
membranes. [Since the toxicity of the
very similar in structure compactin, whose toxicity in animal studies resulted
from it not being tested clinically, that the same occurred for Lovastin, but
Merck went forward. Compactin was withdrawn from the market for ] …
Fortunately,
except for rare cases of myopathy and marked but asymptomatic increases in
hepatic transaminases, none of the adverse effects found in animals occur at
human therapeutic doses.” Nature Reviews
Drug Discovery 2, 517-526 (July
2003) | doi:10.1038/nrd1112
Author’s affiliations: A. Tolbert,
Merck Research Laboratories, Rahway, New Jersey 07065, USA.
Email: jonathan_tobert@merck.com
CHOLESTEROL from http://en.wikipedia.org/wiki/Cholesterol
Cholesterol, from the Ancient
Greek chole- (bile) and stereos (solid) followed
by the chemical suffix -ol for an alcohol,
is an organic molecule.
It is a sterol (ormodified steroid),[3] and an essential structural component of animal cell
membranes that is required to establish proper membrane
permeability and
fluidity. Cholesterol
is thus considered within the class
of lipid molecules.
In addition to its importance within cells, cholesterol also serves as a
precursor for the biosynthesis of steroid
hormones, bile
acids, and vitamin
D.[4] Cholesterol is the principal sterol synthesized
by animals; in vertebrates it is formed predominantly in the liver.
François
Poulletier de la Salle first identified cholesterol in solid form in gallstones in 1769. However, it was not until 1815 that
chemist Michel
Eugène
Chevreul named the
compound "cholesterine".[5][6] Since cholesterol is essential for all animal
life, each cell synthesizes it from simpler molecules, a complex 37-step
process that starts with the intracellular protein enzyme HMG-CoA
reductase [what statins
block]. However, normal and particularly high levels of
fats (including cholesterol) in the blood circulation, depending on how they
are transported within lipoproteins, are
strongly associated with the progression of atherosclerosis. For a man of about 68 kg (150 pounds),
typical total body-cholesterol synthesis is approximately 1 g (1,000 mg)
per day, and total body content is approximately 35 g, primarily located within
the membranes of all the cells of the body. Typical daily dietary intake of
additional cholesterol, in the United States, is 200–300 mg.[7] Most ingested cholesterol is esterified, and
esterified cholesterol is poorly absorbed. The body also compensates for any
absorption of additional cholesterol by reducing cholesterol synthesis.[8] For these reasons, cholesterol intake in food has
little, if any, effect on total body cholesterol content or concentrations of
cholesterol in the blood.
Cholesterol is recycled. The liver excretes it
in a non-esterified form (via bile) into the digestive tract. Typically about
50% of the excreted cholesterol is reabsorbed by the small bowel back into the
bloodstream.
Function[edit]
Cholesterol is required to
build and maintain membranes;
it modulates membrane fluidity over the range of
physiological temperatures. The hydroxyl group
on cholesterol interacts with the polar head
groups of the membrane phospholipids and sphingolipids,
while the bulky steroid and the hydrocarbon chain
are embedded in the membrane, alongside the nonpolar fatty-acid chain of
the other lipids. Through the interaction with the phospholipid fatty-acid
chains, cholesterol increases membrane packing, which reduces membrane
fluidity.[11] The
structure of the tetracyclic ring of cholesterol contributes to the decreased
fluidity of the cell membrane as the molecule is in a trans conformation making
all but the side chain of cholesterol rigid and planar.[12] In
this structural role, cholesterol reduces the permeability of the plasma
membrane to neutral solutes,[13] protons,
(positive hydrogen ions)
and sodium ions.[14]
Within the cell membrane,
cholesterol also functions in
intracellular transport, cell signaling and nerve conduction. Cholesterol is
essential for the structure and function of invaginated caveolae and clathrin-coated
pits, including caveola-dependent and clathrin-dependent endocytosis.
The role of cholesterol in such endocytosis can be investigated by using methyl beta cyclodextrin (MβCD) to
remove cholesterol from the plasma membrane. Recently, cholesterol has also
been implicated in cell signaling processes, assisting in the formation
of lipid rafts in
the plasma membrane. Lipid raft formation brings
receptor proteins in close proximity with high concentrations of second messenger
molecules.[15] Cholesterol
levels can change how quickly surface proteins move within the plasma membrane[16] and
also the efficiency of magnetic capture of cells.[17] In
many neurons, a myelin sheath, rich in cholesterol, since it is derived
from compacted layers of Schwann cell membrane,
provides insulation for more efficient conduction of impulses.[18]
Within cells, cholesterol
is the precursor molecule in several
biochemical pathways. In the liver, cholesterol is converted to bile, which is then stored
in the gallbladder. Bile contains bile salts, which solubilize fats
in the digestive tract and aid in the intestinal absorption of fat molecules as
well as the fat-soluble vitamins, A, D, E,
and K.
Cholesterol is an important precursor molecule for the synthesis of vitamin D
and the steroid hormones, including the adrenal gland hormones cortisol andaldosterone,
as well as the sex hormones progesterone, estrogens,
and testosterone, and their derivatives.[4]
Some research indicates cholesterol may act as an antioxidant.[19]
Dietary
sources
Fat intake
also plays a role in blood-cholesterol levels. This effect is thought[by whom?] to come about by
changes in the quantity of cholesterol and lipoproteins that
are synthesized by the body. Isocalorically
replacing dietary carbohydrates withmonounsaturated and polyunsaturated fats
has been
shown to lower serum LDL and
total
cholesterol levels and increase serum HDL levels,
while
replacing carbohydrates with saturated fat was
shown to increase HDL, LDL, and total
cholesterol levels.[29] Trans fats have
been shown to reduce levels of HDL while
increasing levels of LDL.[30] Based on such
evidence and evidence implicating low HDL and high LDL levels in cardiovascular
disease (see Hypercholesterolemia), many health authorities
advocate reducing LDL cholesterol through
changes in diet in addition to other lifestyle modifications.[31] The USDA, for example, recommends
that those wishing to reduce their cholesterol
through a change in diet should aim to consume less than 7% of their daily
energy needs from saturated fat and fewer than 200 mg of cholesterol per
day.[32] An alternative
view is that any reduction to dietary cholesterol intake could be counteracted
by the organs compensating to try to keep blood cholesterol levels constant.[33] Other research
has found that an increase in the consumption of saturated fats and cholesterol
decreases overall serum cholesterol. [34].
Regulation
of cholesterol synthesis[edit]
Biosynthesis of cholesterol is
directly regulated by the cholesterol levels present, though the homeostatic mechanisms
involved are only partly understood. A higher intake from food leads to a net
decrease in endogenous production, whereas lower intake from food has the
opposite effect. The main regulatory mechanism is the sensing of intracellular cholesterol in the endoplasmic reticulum by the protein SREBP (sterol regulatory element-binding
protein 1 and 2).[37]
Plasma
transport and regulation of absorption
Cholesterol
is transported in the circulatory system
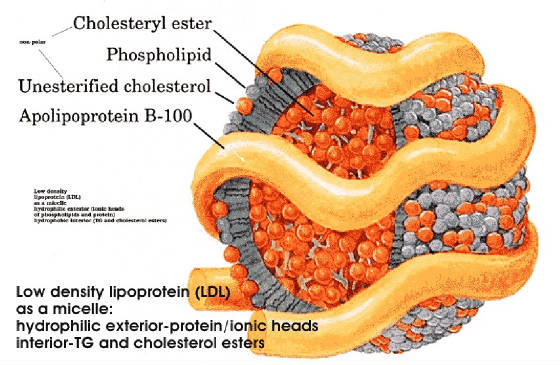
within lipoproteins, complex
discoidal particles that have an exterior composed of amphiphilic proteins
and lipids whose outward-facing surfaces
are water-soluble and inward-facing surfaces are lipid-soluble; triglycerides and
cholesterol esters are carried internally.
Phospholipids and cholesterol, being amphipathic, are transported in the
surface monolayer of the lipoprotein particle.
In addition to providing a soluble means for transporting cholesterol
through the blood, lipoproteins have cell-targeting signals that direct the
lipids they carry to certain tissues. For this reason, there are several types
of lipoproteins in blood, called, in order of increasing density, chylomicrons, very-low-density
lipoprotein (VLDL), intermediate-density
lipoprotein (IDL), low-density lipoprotein (LDL),
and high-density lipoprotein (HDL).
The more
lipid and less protein a lipoprotein has, the less dense it is. VLDL molecules
are produced by the liver and
contain excess triacylglycerol and cholesterol that is not required by the
liver for synthesis of bile acids.
LDL
molecules, therefore, are the major carriers of cholesterol in the blood, and
each one contains approximately 1,500 molecules of cholesterol ester. LDL molecules, therefore, are the major carriers of cholesterol in the
blood, and each one contains approximately 1,500 molecules of cholesterol
ester. Now within the cell, the cholesterol can be used
for membrane biosynthesis or esterified and stored within the cell, so as to
not interfere with cell membranes. These LDL molecules are
oxidized and taken up by macrophages, which become engorged and
form foam cells. These cells often become trapped in the walls of blood vessels and
contribute to atherosclerotic plaque formation. Differences in cholesterol homeostasis
affect
the development of early atherosclerosis (carotid intima-media thickness).[40] These plaques
are the main causes of heart attacks, strokes, and other serious medical
problems, leading to the association of so-called LDL cholesterol (actually a lipoprotein) with
"bad" cholesterol.[39]
HDL
particles are thought to transport cholesterol back to the liver for excretion
or to other tissues that use cholesterol to synthesize hormones in a process
known as reverse
cholesterol transport (RCT).[41] Having large numbers of large HDL particles correlates
with better
health outcomes.[42] In contrast, having small numbers of large HDL particles
is independently
associated with atheromatous disease
progression in the arteries. HDL particles (especially large
HDL) have been identified as
a mechanism by which cholesterol and inflammatory mediators can be removed from
atheroma. Increased concentrations of HDL correlate with lower rates of
atheroma progressions and even regression.
Metabolism,
recycling and excretion
Cholesterol
is oxidized by the liver into a variety of bile acids.[46] These, in turn, are conjugated with glycine, taurine, glucuronic acid, or sulfate. A mixture of conjugated and nonconjugated bile acids, along
with cholesterol itself, is excreted from the liverinto the bile.
Approximately 95% of the bile acids are reabsorbed from the intestines, and the
remainder are lost in the feces.[47] The excretion and reabsorption of bile acids forms
the basis of the enterohepatic
circulation,
which is essential for the digestion and absorption of dietary fats. Under
certain circumstances, when more concentrated, as in the gallbladder, cholesterol crystallises and is the major
constituent of most gallstones.
INTERNAL SITE SEARCH ENGINE by Google
Looking for a topic, use Google Internal Search
Engine
^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^ Remember that
pharma is in the business of treating illness. There claim of preventing illness is in most cases mere marketing.
Disclaimer: The
information, facts, and opinions provided here is not a substitute for
professional advice. It only indicates
what JK believes, does, or would do. Always
consult your primary care physician for medical advice, diagnosis, and
treatment.
|
|
|
