|
Aspirin
(ASA, acetylsalicylic acid)--1/23/2022 http://healthfully.org/rc/id3.html,
on aspirin http://healthfully.org/aspirin/,
/nsaids
Reduces
risk for cancer of Breast 39%,
Colorectal 63%, Esophageal 73%, Hodgkin’s Lymphoma 60%, Ovarian 47%, Melanoma
55%, Prostate 39%, Stomach 62%, and other
cancers including Bladder, Skin, Gastric & Leukemia.
Aspirin increases survival of stages I, II, & III cancers: Breast 66%,
Colon by 74%, and by
extension all adenocarcinomas. Aspirin reduces
the risk of Alzheimer’s Disease
60%, and Heart Attacks 51%, and its
anti-inflammatory action inhibits atherogenesis thus
CVD; Aspirin lowers blood glucose and can reverse both insulin
resistance and type-2 diabetes. with the 350 mg or more, not low dose, see below. Why it prevents most
of the conditions of affluence, see mitochondria heading and first paragraph. Two more summaries of ASA on cancer
protection and on atherosclerosis
protection
Aspirin is natural
in that salicylic acid is widely produced by plants mainly to protect plants from microbial and fungal infestations. As such mammals have, like with vitamins, developed positive uses for salicylic acid. Aspirin is a modified form of salicylic acid to improve its gastric tolerance, which
much later was discovered that it also promotes a major reduction in cancer risk. It
is rapidly hydrolyzed in the digestive system to salicylic acid. Moreover, as an acetate its bioactivity is not diminished. It
is distinguished from all the other NSAIDs in that it lowers the risk of heart attack while the others increase the risk.
The American Heart Association, Consumer Report and others confirm both difference. Simply put, “Take the natural
aspirin rather than a weird unnatural chemical with its various serious side effects, such as naproxen and ibuprofen.” Below you will learn of its many benefits.
A sampling of journal articles on aspirin and the other NSAIDs are to be found at http://healthfully.org/aspirin and http://healthfully.org/nsaid
JK takes a 325 mg aspirin a day--often 2--since 1992 because it reduces risk for cancer, for which we have a lifetime
risk of 50%, and it reduces the risk for Alzheimer’s disease the 4th biggest killer after heart attacks,
strokes, and cancer. It reduces the risk of heart attack by reducing blood clotting. A heart attack and stroke (ischemic events) is a two step process: first leaking young, immature plaque from an artery wall that partially obstructs the flow of blood. The turbulence at the point of partial blockage initiates a blood clotting response. With aspirin and other NSAIDs they block a clotting factor thus reducing or preventing
an acute ischemic event.
For these reasons I am willing
to doubling the risk of an ulcer from 2% to 4%. Moreover, since persistent heart
burn proceeds an ulcer, I would go to the doctor and have my H. pylori eradicated with antibiotics.
Think like a CEO of a big pharma
company, the mandate is to maximize profits. This explains their position on
aspirin, and the reluctance to treat h. pylori.
These numbers above are low: First, the population
that is taking aspirin includes those who are taking low dose, which has been
available since the 1970s as too enteric coated, and the cancer protection is
near zero because of their tolerance to the low dose and poor and delayed
absorption of the coated aspirin. Second
those who take aspirin are a select population whose health is poorer than
those not taking aspirin; thus, to compare their risk to the general population
under-estimates aspirin’s benefits. . Moreover,
the sick and elderly would have less a response to aspirin. Many of them have
arthritic pains, it is a
sign of a fundamental dysfunction on a cellular
level because of
mitochondrial
dysfunction, which puts
then at higher risk for all sorts of conditions
including cancer, and they are sedentary, and such a population of aspirin users
are less like to take hormone replacement, exercise, eat a low sugar diet. The
risks would be less if they were a healthier population to start with. Finally,
reduction depends on duration thus 10
years is better than 5.
This seems
like a drug marketing hype, all those claims, but it isn’t. High
dose aspirin lowers significantly
serum glucose and thereby reduces the percentage of dysfunctional mitochondria
in cells and thus increases the production of the energy molecule ATP. Every
cells and tissue gradually benefit from
the normal amount of ATP. insulin
resistance will diminish and rate of autophagy (healing) increase.
So why doesn’t every-one know of these benefits above, and
why don’t doctors recommend a 325 mgs of uncoated aspirin daily? The
short answer is corporatization
of medicine which includes medical education and
regulatory capture. Pharma profits much more
from illness than it does from creating wellness. As Harvard Prof. Marcia Angell, MD. and former Editor-in-Chief of the NEJM: “If we had set out to design the worst system
that we could imagine, we couldn’t have imagined on as bad as we have” her video. A chorus
of professional critics confirm her
dismal assessment, but you won’t hear them in corporate media. As a social animal physicians and the public have become
true believers.
The evidence for an even longer list of
benefits is in the
next section. These benefits explain
pharma’s multifaceted attack, which includes use of too low a dose (125 mg),
coated aspirin, which takes 5-8 hours to dissolve. Tolerance develops with
low does and coated
aspirin only half is absorbed because it has passed the part of the small
intestines where most would be absorbed, and it takes too long for pain
reduction. The scare about ulcers &
Reyes syndrome (an extremely rare condition in children) is explained below. Pharma’s
assault has turned the #1 NSAID, the first recommended treatment for arthritis
and moderate pain into the 7th, as of 2012.
Besides ignoring its benefits, no mention is
made that aspirin
in its bioactive form of salicylic acid is found in plants as part of their
immune system—yes, plants are attacked by viruses, fungi, and bacteria, and
aspirin is protective for plants and mammals.
There is no mention that we get a moderate amount of aspirin in our diet
depending on amount of vegetables eaten, or that the body synthesizes aspirin
for its anti-pathogen properties—all this is confirmed in a pod
cast by Scientific American. If it
was used as a co-enzyme in an essential pathway it would be classified as a
vitamin, but it is used in non-vital ways that reduce risk for most of the
age-related conditions for those on the western high sugar diet. The reduction
in sales of aspirin is
contributory to many of our illnesses, since its use has been replaced by naproxen,
acetaminophen, and other NSAIDs which promote significantly an assortment of ailments,
including the big one cardiovascular disease. Aspirin clearly should be our
first choice
among supplements. Supplements because it
is part of our diet like vitamins, CoQ10, and minerals. Doe spin’s modus
operandi see ria (below).
“Aspirin elevated ATP levels” at 2002,
and ATP made in the mitochondria is the energy molecule that powers the repair-&
replacements.
The recorded history of aspirin starts with the
ancient Egyptians. The Greeks used an
extract of willow bark and leaves which contain the plant hormone salicylic
acid. “Salicylic acid (SA) plays
a key role in the establishment of resistance to microbial pathogens in many
plants” at. (ASA is rapidly hydrolyzed in the
stomach to salicylic acid, its active form.) Hippocrates, the Greek physician,
420 BC
wrote of its use to relieve extra for pain & fever. The Romans Pliny the
Elder, and later Galen
added its use as skin ulcer treatment.
The drug remained thereafter in the European pharmacopeia, and became
widely used to treat malaria
by the 1760s. In 1853 a German
chemist modified bitter salicylic acid (SA) to the less caustic ASA
by adding an acetate group, and in 1899 the German dye and drug company Bayer
marketed it as aspirin.
“For almost 100 years the salicylates [aspirin
family of drugs] have retained their preeminent position” Goodman and Gilman Pharmacology,
11th Ed, 2006, p. 692. “It
is the standard against which all rheumatoid arthritis medication should be
measured” supra 690. 3.5 gram is the
recommended dose--Merck Manual 1987, p. 960, and same in earlier editions. In
1958 production peaked at 20,000 tons (3
lb. per person). In the late 50s aspirin’s
share of sales fell to the heavily-marketed newer NSAIDs. Following the 1973
discovery that aspirin reduces the incidence of heart attacks (MIs) by
reducing blood clotting (thrombi) that completes occlusion of a coronary
artery when plaque is leaked. By the
1980s it regained its number 1 position, but much of the sales was for too low
a dose for prevent of cancer, MIs, CVD, etc. “Even at 1300 mg/d, [long-term] 8% of subjects were resistant”
AHA to its anticoagulant action (MI
protection). Its biological
half-life is dose dependent---2-3 hours for low dose and up to 15-30 hours for
large doses. About 80 to 90% of aspirin is bound (inactive) to albumin protein
where it is gradually released; while the rest remains in active, ionized
unbound state. From 80 to 100%
is excreted in the urine,
sweat, saliva, and feces. It has
now slipped to 6th in NSAID sales in 2010, and on my bottle are 15
lines of FDA warnings for stomach bleeding and in children Reyes syndrome. Is
the old wisdom and research false? Or is it another example of tobacco science
used to promote illnesses?
Pharma had by late 1980s gained control of research
and production of information. Aspirin the drug of choice by your parents
and grandparents was “shown” to be unsafe in published tobacco studies. Pharma drummed into the publics and physicians’
heads that aspirin is ineffective & frequently causes stomach bleeds,
ulcers, and Reyes Syndrome in children. Capitalism places profits before
people, and
the pharmaceutical industry profits from illness. This 1.2-trillion-dollar industry
can do
pretty much what it wants in our pro-business world. But the older record has
not been erased,
just ignored. In the 11th
Edition of Goodman and Gilman supra 690, “many clinicians favor the use of other
NSAIDs perceived to have better gastrointestinal tolerability, even though this
perception remains unproven by convincing clinical trials”—ASA's
low rate of ulcers. Ulcers is only
one prong of pharma’s attack on a drug which is cheap and prevents
illnesses. Another approach is to change
the dose. To assure that it isn’t
effective for pain they have cut the dose from 1 gram (2 tablets) to start to
325 mgs. And by enteric coating the
aspirin takes too long to be absorbed to relieve pain. And the peak serum level
is one-half of the uncoated aspirin. And
they encourage through the fear of heartburn and ulcer that it be taken with
food—further delaying absorption. “Compared to an uncoated aspirin the start of
absorption with food averaged 0.8 hours, the enteric start averaged 5.9 hours.
For after feeding the time for peak
serum concentration was 2.7 hours, but for the enteric it was 8.9 hours” at 1987. It is most commonly prescribed for heart
attacks based on the Doctor’s Study in the early 80s using uncoated 325
mgs. It works by inhibiting the second
prong of a heart attack: platelets form
a blood clot to completely occlude a partially blocked coronary artery. As for
Reyes syndrome, diagnosis was based on
symptoms, when genetic testing was introduced the number affected dropped to 2
per year. The coated aspirin is modified
in the large intestine to the less active salicylic acid. “Aspirin irreversibly acetylates the platelet enzyme cyclo-oxygenase and
in this way, interrupts the prostaglandin pathway and prevents the
biosynthesis.... however, enteric-coated ASA preparations can be deacetylated
in the gut [where it dissolves] and hence might lack antiplatelet activity….” at
1984. And to prevent a future
generation of users, pharma and later the FDA warned parents about Reyes
syndrome in children. Diagnosis was
based upon symptoms. However, when a
test for Reyes syndrome was developed in the early 90s, and the cases
dramatically dropped, but pharma and the FDA warnings were changed. “Between 1980 and 1997, the number of reported
cases of Reye’s syndrome decreased from 555 cases in 1980 to about 2 cases per
year since 1994… when genetic testing for inborn errors of metabolism…” Moreover
a mechanism of cause is lacking: “in 93%
of the cases a viral infection had occurred in the preceding three-week
period… and no animal model of Reye’s syndrome has been developed with aspirin”
Wiki 2008. This
2008 passage has since been removed by friends of pharma. And
only 55% salicylate detected, 73% viral infection, yet the FDA’s warning
remains on bottles of aspirin against its usage for those under 19, plus gastro-intestinal
irritation and bleeding, thus getting parents and their children onto other
NSAIDs, all of which increase the risk of MIs and lack protections listed
below. The rise in heart attacks,
arthritis, Alzheimer’s disease, ALS, Parkinson’s, and cancer in part results
from the reduction in the use of aspirin (the main cause high carb & fructose diet). Nearly everyone dies earlier thanks to
pharma’s and food manufacturers’ corporate tobacco ethics—profits before
people, tobacco ethics. This is the
business model for pharma, and my website has many more examples. And I stand
on the shoulders of others. For a partial list of them and their efforts,
go to /rg to watch them on YouTube where there is a page of over 300 lectures
and documentaries with links, and also a list of their books. At /rep and /rmbp are
some of their peer reviewed journals articles.
The only conclusion I and others have drawn is that pharma profits from
illness. And as Prof. Ben Goldacre put
it in his Bad Pharma “The
devil is in the details.” Below are the details of the benefits, and
the
alternatives that promote illness.
Relying on Wikipedia the list of side effects for
aspirin, my parent and grandparents, relatives, neighbors were very fortunate not
have conditions now attributed to aspirin, and the doctors must have had mass
delusion. Listed are heart burn, ulcers,
Reyes syndrome, and AERD (aspirin exacerbated respiratory disease). Aspirin
exacerbates gout, and cause tinnitus,
and skin rash. And there is FDA warning
about a high rate of allergic reaction.
Autophagy and age related
conditions (AGES): The gift that gives (to
pharma) is our western high sugar diet, the fructose half of sucrose is a
reactive sugar which through a process
of glycation bonds to proteins
that are imported from the cytosol into the mitochondria, where the
glycated amino acids undergo further reactions which damages the systems within
the mitochondria including their DNA. Mitochondria
are created from imported proteins and fatty acids, thus an abnormally high
amount of glycated fats and proteins results in diminished functions of the
mitochondria. Since mitochondria
supplies nearly all of the energy molecule ATP from ADP and AMP, through
metabolism of pyruvate and acetyl-CoA derived from glucose and fatty acids, the
damage to the mitochondria (mitochondrial
dysfunction) adversely affects nearly every process in the cell. Of
pathogenic significance is the delayed
replacement of collagen, sensitivity to uric acid, elevated insulin (insulin
resistance) and the down regulation of the cellular repair-replacement system
that occur during autophagy, which are downregulated when ATP is low and
insulin resistance. Aspirin reduces the
rate of glycation by reducing blood glucose, which ultimately reduces insulin
resistance and thereby increasing the rate of clearance of glucose and
fructose, and thereby glycation The main
cause of AGES is glycation and fatty
liver causing insulin resistance from excess fructose--see AEGs. “Aspirin has been shown to be a powerful
inhibitor of post-Amadori Maillard reactions” at
2001. This article describes how aspirin
protects the ubiquitous
collagen (connective tissues) from damage by reactive chemicals produced by
metabolism of carbohydrates and fats and by the reactive sugar fructose by
glycation (Maillard reaction), also. This is the modus operandi (preventing
glycation) is the main way that aspirin lowers the risk for so many
different conditions listed below: every
system is working better because of healthier mitochondria. Healthier
mitochondria through increased ATP increases
autophagy. “Aspiring triggers cardo-protective
mitophagy in mice and nematodes.... induction of autophagy by salicylate” at
2018. Autophagy is an umbrella term
for the various cellular ways in which structures are repaired, or if
sufficiently compromised orderly dismantled. Under autophagy’s umbrella
are mitophagy (orderly
dismantling of mitochondria) and apoptosis (the orderly dismantling of cells) for
their replacement. The benefits
generated through the upregulation
of autophagy, like with the male
and female sex hormones, is
long, both hormones and aspirin improve mitochondrial functions especially its
ATP production.
All NSAIDs
(but aspirin) long-term greatly increases risk of MI--American
Heart association warning also
in journal sources by causing
cardiovascular disease through
inhibition of COX-2;
but only high
dose aspirin protects--by 50%.
ALZHEIMER’S
& ALS
reduced 60% by COX-2 inhibition--Neurology, 997; 48: 626-632,
ALS, Swedish twin matching study,
shows low dose and other NSAIDs don’t. “Aspirin (the quintessential acylating pharmacon) can inhibit the
amyloidogenesis of superoxide dismutase (SOD1)…. therapies for diseases linked
to protein self-assembly” 2015 , and by inhibiting excitatory function of glutamate, Science 1996. Note: testosterone
and estradiol also greatly reduce risk. Chronic use of aspirin inhibits beta
amyloid-aggregation [the physical sign of Alzheimer’s], at 2001, by 2x Science 1996. “Current
knowledge and
clinical data indicate that aspirin can be an attractive addition to treatment
regiments for neurodegenerative diseases”. 2016, and mechanism 2002.
Antioxidant
effects: Salicylic
acid’s [SA, active form of aspirin] immune action is through “catalase a common enzyme found
in nearly all living organisms exposed to oxygen…. It is a very important enzyme in protecting the
cell from oxidative
damage by reactive
oxygen species (ROS)… one catalase molecule can convert
approximately 5 million molecules of hydrogen peroxide to water and oxygen each
second… also catalyze various metabolites and toxins,” Wiki. “SA could also
protect plant and mammalian
catalases against inactivation by H2O2 in
vitro “, at. ASA inhibits lipid peroxidation, DNA damage,
NF-kapa B activation and TNF-alpha production at 1999. ROS are the
major cause of age related degenerative diseases. For example ASA
protect fibrinogen. “In cultured
endothelial cells derived from human umbilical vein, aspirin (30–300 μM)
increased heme oxygenase-1 (HO-1) protein levels in a concentration-dependent
fashion up to fivefold over basal levels…. Pretreatment with aspirin or
bilirubin at low micro-molar concentrations protected endothelial cells [on endothelial damage and Wiki]] from
hydrogen peroxide-mediated toxicity…. a novel mechanism by which aspirin
prevents cellular injury under inflammatory conditions and in cardiovascular
disease.” at
2003. This effect was not
demonstrated with other NSAIDs. “The potent antioxidant
property of gentisic acid [ASA metabolite] may partly account for
the anti-atherogenic effects of aspirin”, at
2005. This affects has shown to
protect numerous tissues/organs such as eye lens, preventing cataracts at 1988. Aspirin protects
against the reactive oxygen species produced by sugars and their metabolites (a
process known as glycation). In
my own case I have inherited a gene for
hemochromatosis from my father, and thus absorb a higher than normal rate of
iron. Excessive iron forms crystal that
cause reactive oxygen a cause for many serious conditions. Aspirin increases
the production of ferritin
which stores iron, and thus prevents the formation of iron crystal
precipitates—at 1998.
Anti-inflammatory
“Aspirin can modulate multiple pathogenic
mechanisms implicated in the development of multiple organ dysfunction in
sepsis and ARDS [acute respiratory distress syndrome]” Critical
Care 2015. The effect is “not by
direct inhibition of COX like most other non-steroidal
anti-inflammatory drugs
(NSAIDs) but instead by suppression
of the expression of the enzyme (via a yet-unelucidated
mechanism)” Wiki,
thus unlike the other NSAID which
increase the risk of heart attack by 50% or more, aspirin lowers the risk. “These
findings provide direct in vivo
evidence for an anti-inflammatory action for both aspirin-triggered LXA4 and
LXA4 stable
analogues and their site of action in vivo, at 1987. Aspirin attenuates
beta-caternin/TCF 4 signaling, at 2001. Also inhibits IKK-beta, which prevents
activation of NF-kapaB that downregulates genes involved in the inflammatory
response—Nature 1998. Note, Peter
Gotzsche expresses doubt of NSAIDs ability
to reduce inflammation, and the evidence in support, measurements of finger diameter
is hardly science. For other NSAIDS, I
doubt there is a net benefit from partially block the immune functions of inflammation
and fever. Nature didn’t evolve these highly-preserved
mechanism to reduce survival. Aspirin fine
tunes these immune responses unlike the other NSAIDs, and thereby prevents
the damage caused in the acute phase. It
wide availability through plant sources for plant biological functions explains
its salubrious functions in mammals.
Antimicrobial: Given that pathogens play the major role in cardiovascular disease,
safe antimicrobial agents ought to be widely researched. The lead
starts with plants: because of
salicylic acid ability to inhibit many plant pathogens, this brother of aspirin
is produced in many plants, and thus unlike other NSAIDS animals have developed
uses for this commonly supplied chemical, Plant
Journal 1992, and book 2000. “Aspirin-triggered lipoxin enhances
macrophage [large immune cells] phagocytosis of bacteria [engulfing bacteria]
while inhibiting inflammatory cytokine production” 2011. Inhibits growth
of H. pylori, BMJ Gut, 2017, and clinical
trial 2017. “The
aspirin N‐mustard agent expressed
strong antibacterial activity against a penicillin‐resistant bacteria and
first‐order alkylation kinetics” biotechnology
2003. Like so much of our profits
first world, the trail is thin.
Apoptosis: is the system whereby significantly dysfunction cells are
systematically dismantle for reproeessing of molecules. The process removes
precancerous cells, benign
tumors, and the likes. Aspirin through
the release of cytochrome c from the mitochondria turns up apoptosis--see
cancer below.
Atherogenesis slowed:
“strong evidence that atherosclerosis is slowed down in a dose term” by 47%, stopped, also.
Mechanisms: By NO endothelial cells oxidative damage,
inhibits leukocyte
attacks, cytokinies, CD36,
FFA & diabetes. For papers on developing the use of aspirin
for atherosclerosis and for cancer, and limited value of chemotherapy.
Autophagy, is
the healing
process which aspirin turns up, I
hold the main way is through reducing insulin resistance and mitochondrial
dysfunction, which I develop at http://healthfully.org/rmb/
and elsewhere. Other ways of turning up autophagy is through being a fasting
mimic, 2018
and 2018
full. This promotes apoptosis
of cancer cells, and tissue healing.. I hold that this is down stream of
its upregulation of glucose and decreased mitochondrial dysfunction.
BREAST CANCER SURVIVAL
(long),
UP 67% compared to no aspirin use stages 1-3; by necrosis factor TNF,
and.
Mechanism: COX-2 which increases
prostaglandin which correlates to metastasis and carcinogenesis, which aspirin
blocks.
CANCERS
VARIOUS TISSUES RISK: reduction
of “63% colon, 39% breast, 36% lung, and 39% prostate cancer. Significant
risk reductions were also observed for esophageal 73%, stomach 62%, and ovarian
cancer 47%” also,
and. Epidemiologic studies of malignant melanoma,
Hodgkin's disease, and adult leukemia also found that NSAIDs are protective; melanoma 55%. Other studies have
shown that aspirin promotes the death of abnormal cells through the
natural mechanism of apoptosis by stimulating tumor necrosis
factor NF-B,
by p38
& JNK, mechanism. Long term, but low dose
is insufficient. These numbers are low, allow me to
explain. First, the population that is
taking aspirin includes those who are taking low dose, which has been available
since the 1980s, thus the cancer protection is near zero because of their
tolerance. Second those who take aspirin
are a select population whose health is poorer than those not taking
aspirin. Many of the have arthritic
pain, a sign of a fundamental dysfunction on a cellular level because of mitochondrial dysfunction, which
puts that at higher risk for all sorts of conditions including cancer, and they
are sedentary, and such a population of aspirin users are less like to take
hormone replacement. The risks would be less if they were a healthier population
to start with. Various mechanism why ASA use for cancer therapy, FULL 2011.1993 colon
study.
Cognitive decline
following surgery prevented with aspirin: “ Hospitalization for
major surgery or critical illness often associates with cognitive decline.
Inflammation and dysregulation of the innate immune system can exert broad
effects in the periphery and central nervous system (CNS). . . Systemic
prophylaxis with aspirin-triggered resolvin D1 (AT-RvD1: 7S,8R,17R-trihydroxy-4Z,9E,11E,13Z,15E,19Z-docosahexaenoic
acid, as little as 100 ng dose per mouse) improved memory decline following
surgery and abolished signs of synaptic dysfunction.” 2013
Diabetes
treatment of type 2 (T2D)
with high dose aspirin or other salicylates has a positive effect upon obesity
and diet induced insulin
resistance; thus by improving
the function of insulin it lowers serum glucose
level through improved in glucose
metabolism. Going back over a
century salicylates (aspirins) were used to treat T2D. Noting that “rheumatic fever and diabetes
rarely coexist,… an intensive 2-week course of aspirin [5 gm daily] abolished
glycosuria and lowered the fasting blood sugar to normal… to moderately
severe diabetics” BMJ-1953
also 2001, and review. On low carb diet to treat T2D and
treat non-alcoholic fatty liver disease and reverse Insulin
resistance—see diet articles
at id.14 & id 15.
Drug safer, “The
prevalence of asthma, atopic eczema, and allergic
rhinitis has increased over the last three decades” cause the increase use of acetaminophen replacing aspirin,
at 1998,
Endothelial cells
play a key role in modulating functions of the tissues they form the outer
layer. Aspirins through modulating mitochondrial
functions improves endothelial cell functions, 2002.
Fibrosis of lungs and other tissues (fibrotic scarring): Fibrosis
is a condition that can affect lungs,
liver brain (glia scar) heart and other tissue types. Reduces paraquat-induced
lung toxicity, 2019, risk for fibrosis in patient with NAFLD
(fatty liver) 2019.and lower risk of liver fibrosis 2016, and lowers rate of progression to NASH, 2019. “Aspirin
is a cardioprotective drug with anti-cardiac fibrosis action in vivo” 2017. “Aspirin
inhibits endometrial fibrosis by suppressing TGF-beta1….” 2020.
Cystic fibrosis, 1999. “Aspirin
inhibits NF-kapa-B and protects from angiostein II induced organ damage…
explains utility of high dose aspirin.” 2001
Gout aspirin
in a high does is a uricosuric
drug, increases the secretion of uric acid in the urine; it thereby lowers
the formation of uric acid crystals that cause gout, kidney damage, and
endothelial dysfunction, which is one reason aspirin slows atherogenesis—see SCAm
1991. Also in Alexander Haig’s 1894
book on hyperuricemia, salicylates were used for treatment. Because of the glucose
and fructose lowering
effect, the production of uric acid is reduced by a reduction in the IMP pathway
stimulated by fructose caused by the depletion of NADP.
Heart
attack deaths lowered 51% for higher dose; it
prevents aspirin resistance,
and. A heart attack is a two-step process, first
immature plaque leaks and partially blocks a coronary artery, then platelets
aggregate and form around the partial blockage, and totally obstruct the flow
of blow. Aspirin irreversible blocks
platelet aggregation. This is the
immediate protective effect of aspirin. For unstable
angina, a 236% reduction in death, cardiac event 52% meta-study;
previous MI 2 studies by 44%. Method by artery infection. “Reduction of stroke & death
of 25% to 42% using
900 to 1300 mg aspirin daily” AHA.
Statins block
aspirin. As a powerful antioxidant ASA
protect fibrinogen from oxidation a key clotting factor, thus thereby
reducing the risk of/extent of a clot forming during a MI or other ischemic
event, at
1998. ASA stops
atherosclerosis summary. Enteric
coated aspirin has the acetate group removed in the large intestines where it
dissolves and this prevents the “deacetylated prevents antiplatelet activity,
1984.
Protects endothelial cells, 2020.
Immune
system functions: “aspirin
improve immunoregulatory potential and modulates the innate and
adaptive immune responses.” Upregulates immunomodulatory
relation of aspirin to different immune cells, 2012.
Metabolic
syndrome is a family of conditions causal
for MI that results from the high carbohydrate with sugars western diet,
see CVD. An experiment in fructose fed
rats that were after 6 weeks given aspirin at an equivalent to our 975
mgs. Aspirin reversed all of the signs
of metabolic syndrome: hypertension,
promoted vascular remodeling, reverse insulin resistance, and prevention of
oxidative stress which is causal for endothelial dysfunction, at
2008, 2001 for mechanism.
Mental Illness: There
is compelling evidence to support an aetiological role for inflammation,
oxidative and nitrosative stress (O&NS), and mitochondrial dysfunction in
the pathophysiology of major neuropsychiatric disorders, including depression,
schizophrenia, bipolar disorder, and Alzheimer's disease (AD)… new therapy for
a range of neuropsychiatric disorders, FULL
2013. See above “Alzheimer’s ALS”
risk reduction by ASA.
Mitochondria dysfunction
(MTD) has multiple pathogenic effects of which
probably all the risk can be reduced with regular high dose aspirin. The main
reason is that MD is caused by
excess fructose on the Western diet, the conditions of affluence. Excessive
fructose glycates with proteins,
amino acids and other compounds produced in the endothelium reticulum that are
transported to the mitochondria. The
results of MTD are insulin resistance whose extreme form is type-2
diabetes. By lowering serum glucose,
aspirin reduces the pathogenic effects of fructose. Fructose is metabolized
in the liver after
glucose. By lowering blood level of
glucose, and thus cellular level of glucose the higher dose of aspirin lowers insulin
resistance significantly and thereby the degree of MD, and thus its pathogenic
consequences. This is a slow process of
promoting lower blood and cellular glucose and thereby reducing the percentage
of dysfunctional mitochondria. This is a
brief incomplete summary as to why aspirin has so many varied salubrious
effects. With increased ATP production
in the mitochondria comes in a positive circle the increased rate of repair and
replacement of dysfunctional mitochondria 2013 One example mention in this paper is in reducing the risk of cancer, since the signaling
for apoptosis of abnormal cells is initiated because of signaling by the
mitochondria. This function is affected
by the state of the 100 or more mitochondria in most cell types. This process
of apoptosis prevents cells from
becoming pre-malignant. Much like a
vitamin, but unlike a vitamin aspirin is not an essential cofactor in a vital
process, thus it is like B4, B8, B10, B11, B13, B14, B15, myo-inositol, beta
carnitine, and others other compounds that were classified as a vitamin or
proposed--all failed the standard. Aspirin
MTD effect comes from lowering of blood glucose and thus glycation. Fructose
in excess is a slow acting poison. The development of these conditions is because
of mitochondrial dysfunctions with diabetics having a greater percentage of
dysfunction mitochondria. More direct evidence
is the increase in fatty acid oxidation by the mitochondria
and 1993, and restores ATP level.
Multiple sclerosis (MS): Aspirin (ASA) 1,300 mg/day or placebo
in a
double-blind crossover study. Results favored ASA for the main clinical
outcomes: Modified Fatigue Impact Scale scores (p = 0.043) and
treatment preference (p = 0.012). There
were no significant adverse
effects,” 2005.
“Aspirin should slow or prevent the demyelination of neuron in MS patients by
increasing the expression of cilary neurotrophic factor, “There are several advantages of aspirin over
other available therapies for MS,”
full 2013; and for
a review of 11 different effects of aspirin on MS with links, 2015,
and profoundly affect mitochondrial
metabolism and energy utilization” 2012.
Oxidative
stress
is reduced by aspirin through the mitochondria-lysosome axis. “Preincubation
with aspirin (3–30 μM)
protected endothelial cells from hydrogen peroxide-induced toxicity and
increased viability in a concentration-dependent fashion by up to 64% of
control,” 1997,
and much
more..
Osteoarthritis (OA) a
degenerative joint disease involving degradation of joints including articular
cartilage and subchondral
bone, for which aspirin promotes healing & relieves pain, and
“is the drug of choice” Merck supra 973.
“Aspirin
can inhibit osteoclast differentiation and bone resorption activity in a
dose-dependent manner, thus exerting its anti-osteoporosis effect” at 2013, also,
and, and. ASA has positive effect on bone remodeling.
Pulmonary
embolism following high-risk
surgery, 6%
versus 15.4% placebo--p 231, similar with
1,200 mg, and,
and 3
gm.
Rheumatoid
arthritis (RA) an autoimmune disease causes inflammation
and joint
pain. Merck Manual 1987, p. 960, recommends
a dose “from 3 to 7.5 gm, the average 4.5 gm” for RA. Goodman &
Gilman supra, aspirin is “the
gold standard”
for RA.” As anti-inflammatory drug slows
the auto immune attack, reduces pain, at
while also lowering
the risk for CDV.
Stroke
neuroprotection: “Aspirin
is preventive against stroke not
only because of its antithrombotic properties but also by other direct effects.
The aim of this study was to elucidate its direct neuroprotective effects....
Aspirin inhibited OGD-induced neuronal damage at concentrations lower
(0.3 mmol/L) than those reported to act via inhibition of the transcription
factor nuclear factor-κB (which are >1 mmol/L), an effect that correlated
with the inhibition caused by aspirin on glutamate release” Stroke Journal 2002,and
2002,
and Science 1995,
similar Neuochemistry
2008 and “Aspirin also inhibited ischaemia-induced decrease in brain ATP
levels.” “The neurotoxic effects of the
dopamine‐selective neurotoxin MPTP (15 mg/kg, s.c.), in mice, were totally
prevented by systemic administration of salicylate”, at
2002. Neuroprotective effects of aspirin. . . useful in the
management of patients with high risk of ischemic events; and promotes superior
healing following a stroke at 2002,
and “significant reduction in infarct volume” at Dec 2001
Longevity: A series of experiments have shown
that
aspirin extends median life in C. elegans by
25%--not maximum lifespan. Several
mechanisms have been uncovered and published in numerous journal articles: 1)
effect on inulin like signal through transcription factors
DAF16/FOXO genes, 2) increases catalase and SOD transcripts, and 3) acetylating
about 20% of mitochondrial proteins, and slightly less non-mitochondrial
protein. Median extension also was found
in mice. By using the flat worm gains
from neuro and MI protection are not
present—YouTube, 35
min.
NOTES: bleeds stomach &
stroke: the typical response of a physician or nurse
to a GI bleed is to blame aspirin and ignore other medications. The lifetime
risk of an ulcer goes from 2% to
4% with a daily dose of 1000 mg. The
stomach and intestine lining are protected by a mucus membrane. The Helicobacter
pylori bacteria
causes 80% of GI ulcers
by boring under the mucus membrane. This
permits the stomach’s hydrochloric acid (HCl), digestive bile and drugs
to irritate the lining. However,
digestive bile excreted into the duodenum is basic and neutralize hydrochloric
acid and aspirin. There are four times as many ulcers in the duodenum
than the stomach, thus aspirin is minor causal factor. At 5 years a 22%
increase for 325 mg aspirin (169 ulcers aspirin vs. 138 placebo). The rare hemorrhagic
stroke (1/7) is offset “[net]
reduction of
[stroke] 25% to 42% using 900 to 1300 mg
aspirin daily” AHA.
Tums is best antacid; avoid PPIs,
Anticoagulant drugs Warfarin (Coumadin),
Plavix,
and other have a much higher risk of serious bleeding episodes. Warfarin
accounts for an estimated
33,000 hospital admission for hemorrhaging.
Standard treatment for arrhythmia (fibrillation) includes an
anticoagulant for life, but the vast majority of cases the risk rewards don’t
justify the use (the risk of bleeding increases over the years). And there are
other side effects, including
large red blotches under the skin. Journal
articles down-play bleeding by counting only 2
or more pints of blood. Except for
Warfarin there is no antidote for bleeding, thus pharma’s prescription choice
causes far more deaths. Greater
protection comes from aspirin the Cochrane
Review, and the AHA
agreed. Aspirin
in the medicinal dose of 325-975 mg
is a healthier and safer choice.
For pain and inflammation:
By Pharma exaggerating
the risks and ignoring
benefits, physicians believe there are better alternatives for pain such as Celebrex, a blockbuster
which triples MI risk—band in EU & Canada.
Pharma 30 years ago dropped the dosage to the less effective 325 mg
thereby causing users to switch to heavily advertised alternatives Advil,
Tylenol, and Aleve. The once standard 1,000 mgs to start and 500
mg is dose comparable to Advil & Alive.
Studies justify the higher
dose of 900-1,300
mg. Enteric coated takes hours to
dissolve, thus not for prompt relief, not
for pain and 8.9 hrs.
with food. There is no advantage from adding an
NSAID to an opioid analgesic, except for inflammation.
Aspirin (salicylic acid)[1] is natural: These
benefits occur because
aspirin (salicylic acid) has evolved salubrious biological functions. Plants
make salicylic acid to fight infects
and so do mammals including humans—see,
and. “A
13C6 benzoic
acid
load ingested by six volunteers led, between 8 and 16 h, to a median 33.9%
labeling of urinary salicyluric acid. The overall contribution of benzoic acid
(and its salts) to the turnover of circulating SA [salicylic acid] thus
requires further assessment” Nov 2008. The production of salicyluric acid is an
excretion for of salicylic acid, thus the benzoic acid has been converted. This
shows a conversion of benzoic acid into
the active form of salicylic acid. Given
the complex of mammals’ biological systems, like with so many other hormones
and simple compounds, mammals have evolved multiple functions for salicylic acid. Because
it is found in most of the plants we
eat as part of their immune system, mammals evolved similar functions for
salicylic acid as it has for vitamins; it is thus quite safe. The claim for
“aspirin intolerance” is based
up the development of hives
within 3 hours of taking aspirin; however, given the long list of causes
for hives, the belief pharma has drummed into to doctors and nurses of
aspirin’s role, rather than their patented drugs, the manifestation of
intolerance is grossly over reported.
Moreover, salicylic acid is common to plants, thus such reaction given
long-term dietary exposure makes this claim even more suspect.
Fat soluble form
has better effects
“Prior to the synthesis of new aspirin derivatives, we assessed whether generic
aspirin can be incorporated in the hydrophobic core of biodegradable
polymeric NPs. As we would like to target conditions such as
mitochondrial dysfunctions associated with oxidative stress, impaired Ca2+ signaling, inflammatory processes
demonstrated by brain cells during neurodegenerative processes, we selected a
biodegradable poly(lactic-co-glycolic acid)-block-polyethyleneglycol (PLGA-b-PEG)
polymer functionalized with a terminal triphenylphosphonium cation (TPP) with
significant mitochondrial association properties.” 2016
[1]
Acetylsalicylic acid (aspirin) is readily converted (hydrolyzed) in the stomach
to salicylic acid, and in this form is bio-active.
^^^^^^^^^^^^^^^^^^^^^^ Non-technical summation^^^^^^^^^^^^^^^^^^^^
Aspirin: In the
1950s, when I was growing
up, aspirin was the dominant over-the-counter drug for mild pain, arthritis, anti-inflammatory,
and colds. It came in 500 mgs,
and the initial dose was 2, followed by 1 every 3 hours, or as needed. The standard
daily usage for arthritic and
joint pain, and chronic lower back pain was 2.5 grams per day, with 7.5
grams as the upper limit—this continued to be recommended by doctors until the
1990s. Annual production reached a peak
in the U.S. of 20,000 tons in 1958. Nothing
has changes since the 1960s as to its risk factors, and several major benefits
were added including those of reduction of heart attacks, cancer prevention,
and increased cancer survival, yet its sales have decline until now it is 8th
among over-the counter pain medications.
Given that the American Heart Association warns that all NSAIDs[1]
but aspirin increases significantly the risk of heart attack, this is proof
of their affect of pharma upon doctors and the public. Among it significant
benefits are prevention
of hardening of the arteries, cancer, Alzheimer’s disease, and thrombosis
especially those which result in heart attacks and strokes. Aspirin reduces
the yearly risk of the top
three killers. Because of its anti-inflammatory
action, “It is the standard against which all rheumatoid arthritis
medication should be measured” Goodman & Gilman 11th
Ed,
2006. Promotes healing of osteoarthritis
and is drug of choice Merck 15th Ed. p 973. Aspirin’s anti-inflammatory action & prevention
of oxidative damage prevents hardening of the arteries, which is essentially an
inflammatory process to oxidized LDL (see hardening of the arteries below). Aspirin
also promotes the death of abnormal
cells by stimulating the body’s mechanism for destruction of abnormal cells
(necrosis factor) including trauma damaged cells and precancerous tumors
cells. By doing so it both prevents most
cancers and promotes survival For example,
with breast cancer the rate is reduced over 40% and survival of stages I, II
& III increased over 60% (doesn’t affect metastatic cancers. Pharma
thus attacks the usage aspirin because
it would drastically reduce the sales of nearly half their blockbusters. Besides
ignoring aspirin’s benefits, pharma
has blown out of proportion its health risks.
Doctors automatically blame all major & minor bleeding episodes on
aspirin, though scientific studies shown to increase risk about 4% for an ulcer
over 5 years. They fail to consider the
concurrent drugs and Helicobacter pylori bacteria as causes. Goodman and Gilman
supra, comment that “many
clinicians favor the use of other NSAIDs perceived to have better gastrointestinal
tolerability, even though this perception remains unproven by convincing
clinical trial”. And to prevent the
next generation pharma and the FDA warn about Reyes Syndrome. Once diagnosed
based on symptom with 555
cases in 1980, it dropped to two cases in 1994 with the advent of genetic
testing for a metabolic syndrome. This
drop in frequency is ignored by pharma and the pharma friendly FDA, they
continue to warn about Reye’s syndrome.
Finally on dosage: pharma reduce
the pill from 500 mgs to 325, and initial dose from 1 gram to 325 mg, which is
too low to be effective for pain. And to
insure it being ineffective they coated the aspirin (enteric) so that it
doesn’t peak level isn’t 5 hours and 8.9 hours with food. The delay entails a
much lower level of absorption, at 1987. The older journal literature shows that
aspirin benefits more than justify its risks.
Effective doses are daily 325 to 650 mg for protection; 2.5 grams daily
for pain reduction and arthritis and treatment of thrombosis (see anticoagulant). Finally aspirin is natural: it is produced both by plants and mammals as
salicylic acid to fight infections. Thus
for mammals with their complex
bio-systems, salicylic acids has evolved multiple functions with minimal side
effects.
^^^^^^^^^^^^^^^^^^^^^^^^^^^
Eleven Reasons why I take aspirin, why pharma
should be limited. 1) Aspirin lowers
risk of Alzheimer’s disease. 2)
Aspirin increases survival of
stage I, II, AND III adenocarcinoma by over 60%. 3) Lowers risk
of most cancers over 30% through destruction of abnormal cells, thus lowers the
risk for precancerous polyps and other tumors.
4) Alternatives NSAIDs have far worse side effects than aspirin AHA warns. Except for aspirin, all
prescription and over-the-counter NSAIDs with long term usage greatly increase
the risk of myocardial infarction (MI)
and cardiovascular disease repeatedly
warns
the American Heart Association
because they prolong the
formation of plaque once the process starts.
In the APPROVe Study Naproxen increased 50% and Vioxx 300% heart
attacks.[2]
Celebrex is still on
the market. 5) the second step in a
myocardial infarction is the formation of a blood clot cutting of oxygen to the
heart muscle, and aspirin blocks that formation by its affect upon
platelets. 6) Prevents atherogenesis
thus cardiovascular disease the basis for most heart attacks by reducing the
inflammation response. 7) Powerful antioxidant. 8) Lowers the risk for Alzheimer’s
disease,
other types of dementia, and Parkinson’s disease. 9) Prevents type-2 diabetes
by lowering the
level of glucose in the blood, and has been used to treat t2d. 10) by lowering
blood levels to glucose it
reduces the risk of development of fatty liver, metabolic syndrome, and the age
related conditions associated with the western diet. 11) Use of anticoagulants Warfarin, Plavix, et al to prevent
venous embolism and MI are inferior to full dose aspirin and
they caused thousands of major bleeding episodes.
[1] NSAID are None
Steroidal Anti-Inflammatory Drug, this
includes naproxen in Aleve, ibuprofen, Celebrex, and over 30 others. Naproxen,
for example, has been shown when
taken long-term to increase the risk of heart attacks at least 50% and Celebrex
200%, yet both are widely prescribed for arthritis. Vioxx was voluntarily removed
by Merck when
it was shown to increase the death rate from heart attacks by 400% in a study
on the prevention of Alzheimer’s disease.
[2] “An FDA analyst
estimated that Vioxx caused between 88,000 and 139,000 heart attacks, 30 to 40
percent of which were probably fatal, in the five years the drug was on the
market.” Studies show a much greater association with higher does
given over 2 years (over 3-fold)—as in the treatment of arthritic pain. After
discontinuation of Vioxx, the risk of
event would continue to be greater than the control group.
For more on aspirin and NSAIDs go to NSAIDS and ASPIRIN: THE BEST NSAID
|
|
^^^^^^^^^^^^^^^^^^^^^^^^^^^
Eleven Reasons why I take aspirin, why pharma
should be limited. 1) Aspirin lowers
risk of Alzheimer’s disease. 2)
Aspirin increases survival of
stage I, II, AND III adenocarcinoma by over 60%. 3) Lowers risk
of most cancers over 30% through destruction of abnormal cells, thus lowers the
risk for precancerous polyps and other tumors.
4) Alternatives NSAIDs have far worse side effects than aspirin AHA warns. Except for aspirin, all
prescription and over-the-counter NSAIDs with long term usage greatly increase
the risk of myocardial infarction (MI)
and cardiovascular disease repeatedly
warns
the American Heart Association
because they prolong the
formation of plaque once the process starts.
In the APPROVe Study Naproxen increased 50% and Vioxx 300% heart
attacks.[1]
Celebrex is still on
the market. 5) the second step in a
myocardial infarction is the formation of a blood clot cutting of oxygen to the
heart muscle, and aspirin blocks that formation by its affect upon
platelets. 6) Prevents atherogenesis
thus cardiovascular disease the basis for most heart attacks by reducing the
inflammation response. 7) Powerful antioxidant. 8) Lowers the risk for Alzheimer’s
disease,
other types of dementia, and Parkinson’s disease. 9) Prevents type-2 diabetes
by lowering the
level of glucose in the blood, and has been used to treat t2d. 10) by lowering
blood levels to glucose it
reduces the risk of development of fatty liver, metabolic syndrome, and the age
related conditions associated with the western diet. 11) Use of anticoagulants Warfarin, Plavix, et al to prevent
venous embolism and MI are inferior to full dose aspirin and
they caused thousands of major bleeding episodes.
[1] “An FDA analyst
estimated that Vioxx caused between 88,000 and 139,000 heart attacks, 30 to 40
percent of which were probably fatal, in the five years the drug was on the
market.” Studies show a much greater association with higher does
given over 2 years (over 3-fold)—as in the treatment of arthritic pain. After
discontinuation of Vioxx, the risk of
event would continue to be greater than the control group.
“The
pharmaceutical industry is the most lucrative, the most cynical and the least
ethical of all the industries," Dr. Philippe Even tells The Guardian.
"It is
like an octopus with tentacles that has infiltrated all the decision-making
bodies: world health organizations,
government agencies, parliaments, high administrations in health and hospitals
and the medical profession." Author
of "The Guide to the 4,000 Useful,
Useless or Dangerous Medicines" http://www.fiercepharma.com/story/official-french-report-trashes-pharma-calls-many-drugs-useless/2012-09-14
Basic fact: 4 times as many duodenum ulcers as
stomach ulcer. Helicobacter pylori is
the cause of 90% of duodenum and 60% of stomach ulcer. 10-20% of adults that
have chronic pylori
infection will develop an ulcer.

Peptic ulcers: an ulcer of
the duodenum, esophagus, or stomach. Common
errors are made by doctors and nurses, and repeated by the public based on marketing science and
education by the pharmaceutical
industry, hereafter referred to as PhARMA.
The typical response of a physician or nurse to a patient concern over
heart-burn is for them to blame aspirin
(or other NSAID) when possible. PhARMA
and its thought leaders have trained physicians and nurses to blame the
non-prescription drugs for this side effect of medication (please read the
above link on the state of corporate medicine).
PhARMA teach that the NSAIDs anti-platelet effect through COX-1
inhibition, which reducing blood clotting, that this is the causes the, stomach
lesions, bleeding, and ulcers. More
frequently they hear the simple message that aspirin causes ulcer. But this
conflicts with the underlying
mechanism, and lack convincing research.”[1]
Over 80%
of peptic ulcers are caused by chronic colonization in the stomach
by the Helicobacter pylori bacteria
that cause chronic inflammation by colonizing under the mucus membrane which
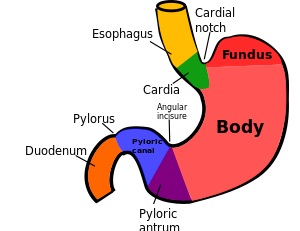
protects the stomach. Most of the peptic
ulcer arises for pylori colonization in the pyloric
antrum, which is the last portion of the stomach, just prior to the
pyloric sphincter at the entrance to the duodenum.[2] See
illustration above. This resulting
inflammation is called “gastritis”, which causes a defect in the regulation of
gastrin. Gastrin regulates the
production of hydrochloric acid (HCl), and this plyori-induced defect causes
too much acid, thus making the stomach too acidic, even when empty. Individuals infected with H. pylori have a 10 to 20% lifetime risk of developing peptic
ulcers and
a 1 to 2% risk of acquiring stomach
cancer.[8]
The type of ulcer depends upon which portion of the stomach the chronic
infection is found: in the pyloric
antrum is more likely to lead to duodenum, and the corpus (body) portion to a
body portion of the stomach (gastric ulcer).
“Four
times as many peptic ulcers arise in the duodenum (the first part of the small intestine just after the stomach)
as in the stomach itself.” The stomach produces hydrochloric
acid (HCl); the duodenum uses enzymes to breakdown food. The pylori bacteria
alone is sufficient to
cause a peptic ulcer; some drugs simply increase the risk, similar in a way to
that of hot peppers and alcohol. These drugs are caustic will irritate the
stomach lining once the mucus membrane has been compromised by the pylori
bacteria. Increased risk of ulcers from
the use of NSAIDs is a result of surface irritation.
PhARMA in changing
the prescription practice
of doctors’ first sold doctors on the grave risks associated with aspirin as to
peptic ulcers and Reyes Syndrome in the 70s.
In the 50s through the 70s aspirin was the most popular of arthritic
medications. This attack on aspirin
helped them sell their palliative, patented arthritic drugs. In addition the
shift promoted their
meg-block buster Plavix,[3] Warfarin and other
blood thinners for
those with high risk for a heart attack or venous thrombosis. They persuaded
doctors to prescribe these
then patented drugs as being safer and more effective.[4]
The shift also promoted sales of their patented NSAIDS. They also pushed
through the media the
over-the-counter more expensive NSAIDs with direct to consumer advertising,
which has always been legal. When Vioxx
(1999) and other COX-2 inhibitors were approved the FDA, doctors already were
trained not to recommend aspirin except in the low dose 82 mgs for those who
would take the patented Plavix or its competitors. By then (permitted in 1997)
direct to
consumer advertise created a demand for these selective COX inhibitors (the
common label for this family of COX-2 inhibitor drugs). Now all PhARMA needed
to do is persuade
doctors that the selective COX inhibitors were both safer and more effective. With
their control of the production of
information that was quickly accomplished.
They told doctors that the selective COX-2 inhibitors since they don’t
affect palliate production, they don’t increase the risk of peptic ulcers like
the other non-selective NSAIDs. As
argued above, platelet inhibition does not increase the risk for dyspepsia
(impaired digestion) and ulcers, but rather the corrosiveness of the drug
itself.[5]
The conscientious physician thus would warn their patients about the
non-selective NSAIDS causing indigestion and peptic ulcers, and then sold them
on the safer and more effective selective COX-2 inhibitors such as Vioxx and
Celebrex. This ploy worked and $10’s of
billions were sold of these drugs.
However, the perceived benefits over aspirin were never convincingly
demonstrated as Goodman and Gilman (supra) wrote. Moreover, they weren’t
safer for all COX-2
inhibitors, but aspirin promote atherogenesis and thus heart attacks,
the selective ones by far the most. Vioxx
in its 5 years before Merck took it off the market, Vioxx
caused an estimated 125,000 heart attacks and 55,000 deaths. Celebrex, which
has the same affect but to a lesser
degree, is still widely advertised, though the FDA advisory panel unanimously
recommended that its direct-to-consumer advertising be barred. As noted in the
footnote Celebrex increases
the risk o f thrombosis, hypertension, and accelerated atherogenesis.
The bottom line is that one should NOT put a strange, unnatural
chemical in your body unless it resembles one that the body normally encounters
and has been shown through long usage to be safe; except of course if the
condition it is to treat is severe enough to merit the risk. Opiates are a family
of drugs that are
extremely safe. And long-term usage is
both safe and non-addicting, unless one takes it in sufficient amounts on a
daily basis to become intoxicated. If
the pain isn’t severe, grin and bear it.
Reaching for an NSAID for minor pain is based on a false perception of
safety, they all increase the rate of cardiovascular disease and it consequences. The
only exception is aspirin, which protects
against cardiovascular disease, MI, and reduces the risk of cancer very
significantly, and promotes survival of early stages of cancer, and reduces the
risk of Alzheimer’s disease. For
dyspepsia there are over-the-counter antacids such as Tums. Even the seeming
inoxious acetaminophen (Tylenol)
has dire consequences. The use of proton
pump inhibitors have made the do-not take list of Worst Pill for good
reasons. The long-term risk of ulcer for
aspirin users is about 4%, about twice that of non-users. JK finds it
worth the risk, and has been
taking 325 mgs since 1991, when a doctor recommended 2,500 mgs per day.
1[6] In
the leading
pharmacology textbook, Goodman and Gilman the Pharmacological Basis of Therapeutics, 11th Ed. 2006, p. 690: “Many clinicians favor the use of other
NSAIDs perceived to have better gastrointestinal tolerability, even though this
perception remains unproven by convincing clinical trials.”
2[7] The sphincter
contracts to
close off the stomach so that it doesn’t drain into the duodenum while the food
is digesting in the stomach. It opens 2-3 hours later.
This delay provides a way for distinguishing
the more common duodenum ulcer from that of the stomach based upon when pain
occurs, with meal or hours later. The
HCL about 0.5% causes the protein to unravel so that digestive enzymes in the
duodenum can break down the long chains into amino acids for absorption.
3[8] Plavix is the 2nd most profitable
drug, after Lipitor,
with world-wide sales as of 2007 of $60 billion.
4[9] This was accomplished head-to-head testing a
low dose aspirin to
their patented products. Moreover , the
very unscientific (without testing) habit of doctors automatically attribute a
hospital emergency from GI (gastro-intestinal) distress as being caused by the
NSAID (other than the selective COX inhibitors) entails that most of such
events are reported as a result of the NSAID, rather than the other medication,
or combinations of medications. Many
seniors are taking 6 or more drugs, plus an assortment of over-the counter
vitamins and herbs. Moreover studies
funded by PhARMA attribute all stomach irritation to the NSAIDs. For an example
of how bad it gets,
5[10] This
was born out in a
review of the evidence by Goodman and Gilman authors on the section on
Celebrex which compared the family of
tNSAID (traditional NSAIDS) to the selective COX-2 inhibitors: “None of
the coxibs [selective COX-2
inhibitors] has established clinical efficacy over tNSAIDS, while celecoxib
[Celebrex] failed to establish superiority over tNSAIDS in reducing
gatro0intestinal adverse events. While
selective COX-2 inhibitors do not interact to prevent the anti-platelet effect
of aspirin…. Current evidence does not support use of coxib as a first choice
among the tNSAIDS… {because of] the risk of thrombosis, hypertension, and
accelerated atherogenesis are mechanically integrated” (supra. 704).
From
Wikipedia:
The pathophysiology
of the H. pylori
centers on its thwarting the stomach’s protective acid environment. “To colonize the stomach, H. pylori must survive the
acidic pH of the lumen and use
its flagella
to burrow into the mucus to reach
its niche, close
to the
stomach's epithelial cell layer.[23] Many bacteria
can be
found deep in the mucus, which is continuously secreted by mucus-secreting
cells and removed on the luminal side. To avoid being carried into the lumen, H. pylori senses the pH gradient
within the mucus layer by chemotaxis and swims
away from
the acidic contents of the lumen towards the more neutral pH environment of the
epithelial cell surface.[24] H. pylori is also found on the
inner surface of the stomach epithelial cells and occasionally
inside epithelial cells.[25] It produces adhesins which
bind to
membrane-associated lipids and carbohydrates and help
it adhere to
epithelial cells. For example, the adhesin BabA binds to the Lewis b antigen displayed
on the
surface of stomach epithelial cells.[26] H. pylori produces large amounts
of the enzyme urease, molecules
of which are localized inside and
outside of the bacterium. Urease breaks down urea (which
is normally
secreted into the stomach) to carbon dioxide and ammonia. The
ammonia is converted to ammonium by
accepting a proton (H+), which neutralizes gastric acid. The
survival of H. pylori in the acidic stomach is
dependent on urease. The ammonia produced is toxic to the epithelial cells,
and, along with the other products of H. pylori—including proteases, vacuolating
cytotoxin A (VacA), and certain phospholipases—,
damages those
cells.[27]
Inflammatory
processes
of H. pylori infections are also
mediated by highly disulfide-bridged proteins. Helicobacter cysteine-rich
proteins (Hcp), particularly HcpA (hp0211), triggers an immune response through
the differentiation of human myeloid Thp1 monocytes intomacrophages. In analogy to eukaryotic cytokines, they
interfere with
host cell functions and change the morphology of monocytes, inducing the
expression of the surface marker protein CD11b, phagocytic activity,
as well as
cell adherence, which are indicative of monocyte differentiation into
macrophages.[28] Colonization of the
stomach by H. pylori results in chronic
gastritis, an inflammation of the stomach lining. The severity of the
inflammation is likely to underlie H. pylori-related diseases.[29] Duodenal and stomach
ulcers
result when the consequences of inflammation allow the acid and pepsin in the
stomach lumen to
overwhelm the mechanisms that protect the stomach and duodenal mucosa from
these caustic substances. The type of
ulcer that develops depends on the location of chronic gastritis, which occurs
at the site of H. pylori colonization.[30] The acidity
within the
stomach lumen affects the colonization pattern of H. pylori, and therefore
ultimately determines whether a duodenal or gastric ulcer will form. In people producing large amounts of
acid, H. pylori colonizes theantrum of the stomach to avoid the acid-secreting parietal
cells located in the corpus (main body) of the stomach.[8] The inflammatory response to the
bacteria induces G
cells in the antrum to secrete the hormone gastrin, which travels
through the bloodstream
to the corpus.[31] Gastrin stimulates the parietal cells
in the corpus to secrete even more acid into the stomach lumen. Chronically
increased gastrin levels eventually cause the number of parietal cells to also
increase, further escalating the amount of acid secreted.[32] The increased acid load damages the duodenum,
and ulceration may eventually result. In contrast, gastric ulcers are often
associated with normal or reduced gastric acid production, suggesting the
mechanisms that protect the gastric mucosa are defective.[32] In these patients, H. pylori can also colonize the corpus of the
stomach, where the acid-secreting parietal
cells are located. However chronic
inflammation induced by the bacteria causes further reduction of acid
production and, eventually, atrophy of the stomach lining, which may lead
to gastric ulcer and increases the risk for stomach
cancer.[33]
About 50–70% of H. pylori strains in Western countries carry the cag pathogenicity island (cag PAI).[34] Western patients infected with strains
carrying the cag PAI have a stronger inflammatory response
in the stomach and are at a greater risk of developing peptic ulcers or stomach
cancer than those infected with strains lacking the island.[8] Following attachment of H. pylori to stomach epithelial cells, the type
IV
secretion system expressed by the cag PAI "injects" the inflammation-inducing agent, peptidoglycan,
from their own cell
wall into the epithelial cells. The injected
peptidoglycan is recognized by the cytoplasmic pattern
recognition receptor (immune sensor) Nod1, which then stimulates
expression of cytokines that promote inflammation.[35]
The type IV secretion apparatus also injects the cag PAI-encoded protein CagA into the stomach's
epithelial cells, where it disrupts thecytoskeleton, adherence to
adjacent cells,
intracellular signaling, cell
polarity, and other cellular
activities.[36] Once inside the cell, the CagA protein
is phosphorylated on tyrosine
residues by a host cell membrane-associated tyrosine
kinase (TK). CagA then allosterically
activates protein
tyrosine phosphatase/protooncogene Shp2.[37] Pathogenic strains of H. pylori have been shown to activate theepidermal
growth factor receptor (EGFR), a membrane
protein with a tyrosine kinase domain. Activation
of the EGFR by H. pylori is associated with altered signal
transduction and gene
expression in host epithelial cells that may
contribute to pathogenesis. It has also been suggested that a C-terminal region of the CagA protein (amino acids
873–1002) can regulate host cell gene
transcription, independent
of protein tyrosine phosphorylation.[21][22] There is a great deal of diversity
between strains of H. pylori, and the strain with which one is
infected is predictive of the outcome.
Two related mechanisms by which H. pylori could promote cancer are under investigation. One mechanism
involves the enhanced production of free
radicals near H. pylori and an increased rate of host cell mutation. The other proposed
mechanism has been
called a "perigenetic pathway",[38] and involves enhancement of the
transformed host cell phenotype by means of alterations in cell proteins, such as adhesion proteins. H. pylori has been proposed to induce inflammation and locally high levels of TNF-α and/or interleukin
6 (IL-6). According to the proposed
perigenetic mechanism, inflammation-associated signaling molecules, such as
TNF-α, can alter gastric epithelial cell adhesion and lead to the dispersion
and migration of mutated epithelial cells without the need for additional
mutations intumor
suppressor genes, such as genes
that code for cell adhesion proteins.[39]
Mechanism
by which
Helicobacter pylori potentiates the effect of aspirin. Namely aspirin and other
drugs are irritants
to the lining of the stomach. Within a
few days the adaptive healing process kicks in, however in the presence of H. pylori,
it does do so adequately. Pylori
bacteria is the cause for GI problems with drugs.
Journal of Physiology
and Pharmacolog: an Official
Journal
of the Polish Physiological Society [1997, 48(1):3-42]
http://europepmc.org/abstract/MED/9098824
Physiological, immunohistochemical
and molecular
aspects of gastric adaptation to stress, aspirin and to H. pylori-derived
gastrotoxins
Konturek PC Department of Medicine I,
University of Erlangen-Nuremberg, Germany.
Abstract:
Gastric mucosa is
continuously exposed to various aggressive factors such as stress, ulcerogenic
drugs including aspirin-like agents, gastro-toxic bacteria,
particularly Helicobacter
pylori (Hp) and many other exogenous and endogenous
irritants. The maintenance of mucosal barrier depends upon the activation of
pre-epithelial (mucus-alkaline secretion),
epithelial (surface active phospholipids,
mucosal cell restitution and proliferation) and
post-epithelial (mucosal microcirculation) lines of mucosal defense. The mucosa
exposed to aggressive factors develops acute lesions, which usually heal
completely within few days, but following repeated exposures to hostile
environment it adapts to survive the challenge of noxious agents. This
adaptation may be of short term (adaptive cyto-protection) and follows the
exposure to "mild" irritants that activate local mucosal biosynthesis of protective prostaglandins (PG) and nitric oxide (NO) and stimulate sensory nerves and mucosal cell
migration and proliferation through enhanced expression of
growth factors such as EGF, TGF
alpha and trefoil peptides.
The fact that exogenous PG, NO-donor agents,
growth factors and capsaicin,
stimulating sensory nerves, protect the mucosa
against strong necrotizing agents (direct cyto-protection), supports the notion
that endogenous PG, NO, growth factors and sensory nerves are involved in the
complex process of adaptive cyto-protection. With repeated insults of
ulcerogens such as stress aspirin, Hp-derived gastro-toxins, especially
ammonia, a long-term adaptation develops which is mediated mainly by over expression
of EGF and TGF
alpha and their common receptor (EGFR)
with subsequent increase of mucosal cell
proliferation
and
enhanced healing of mucosal lesions. The
failure of mucosal adaptation seems to play a pivotal role in the pathogenesis of gastric
lesions and peptic
ulcerations.
|