|
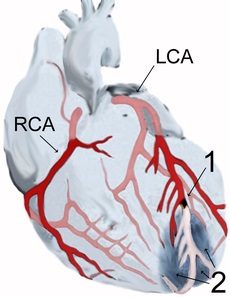
| Coronary arteries shows damage to heart from |
|
| a blocked coronary artery |
Read carefully the material on corporate medicine, then you will understand
what I would do if experiencing an AMI, or had CVD.
Abbreviations
|
AMI Acute myocardial infarction |
|
KOL Key opinion leader |
|
AS Atherosclerosis |
|
MI
Myocardial infarction |
|
CVD Cardiovascular disease |
|
PCI Angioplasty |
Nontechnical Summation on Heart Attack and Treatments What I would do if I
had an AMI http://healthfully.org/rc/id11.html 5/23/16
A 33-page version of this with links to justify findings at
http://healthfully.org/rhi/id1.html
For my qualifications click on JK’s academic background
1) Heart Attacks (MI) and bad pharma: “Each year [2005] 1.5 million Americans experience a heart attack and nearly
460,000 are fatal. Of those who die, almost half die suddenly, before they can
get to a hospital” AHA. Unfortunately, the list of standard treatments for CVD and AMI (listed in clinical guidelines),
are not worth the side effects. How is this possible? It starts with
the fiduciary responsibility of corporations, To give it the right aroma, I call it tobacco ethics. And pharma to maximize
profits uses tobacco science. Thus as Prof. Ben Goldacre
says, referring to pharma and the corporate imperative: “A perverse system
produces perverse result”. Allow me to outline the salient points. There is a seamless connection between bad pharma and the practice of medicine. Key Opinion Leaders, (KOLs), selected
and financially reward by pharma, play a pivotal role. These top figures in their
specialties write the medical textbooks which form the core for university medical training; they run the clinical trials,
they write or signoff on the journal articles on the trials, they give the mandated continuing medical education (CME)
classes which are funded by pharma thus are free to physicians, they write the treatment guidelines, and they occupy key administrative
positions. For this they are on an average receiving over $100,000 per year for services—they are not employed by pharma.
The 800 billion dollar gorilla has captured the regulatory system. The
corporate media deceives the public with spun information. This confluence of
processes explains why physicians give junk treatments.
Pharma having this ability has framed our understanding of medical conditions
and their treatments so as to fill their fiduciary obligations. Their claimed
miracles, aren’t. Medicine lost its way in the corporate-honor period,
beginning under Regan. Now just about every clinical trial is designed
to promote sales. Bias is good for business.
The average positive bias is 32%. When this bias is subtracted from trial
results very few drugs are worth their side effects. Pharma’s mantra of safe
and effective has created a chorus of critical professors. They have exposed pharma’s tobacco science. My posted Video Library
has both a short description plus links to YouTube; it contains what is rarely mentioned in the corporate media. One more point, the major improvement in management of CVD
and AMI has come through 1) reduction in use of tobacco from 46% in 1960 to 16%
today, 2) resuscitation during cardiac arrest and defibrillation during life-threatening arrhythmia, and 3) the use of anticoagulants
in the high risk populations—end of list.
2)
There is a revolt among doctors over the corruption of a once noble profession. The AllTrials,
Centre for Evidence-Based Medicine
(Oxford University with over 25 active staff and honorary members), and the Cochrane Collaboration
which has over 37,000 volunteers, are examples of the growing opposition to corruption worked by pharma. There is a chorus of critics who meet the highest academic standards and publish articles in the leading
journals (including the JAMA (Journal of American Medical), NEJM (New England Journal of Medicine), BMJ (British medical Journal)
and The Lancet. Nearly every issue has an article or two. They have written books
attempting to inform the public and their fellow doctors. Most of their books
are on the cholesterol myth
(refuting industry and government claims that cholesterol and saturated fats are artery clogging); on the Western diet;
in particular the harm done by the combination of sugar (fructose) and refined carbs, the dietary fix for type-2 diabetes;
bad regulators
and bad pharma;
and that psychiatric drugs rather than improving behavior exacerbates the problem because contrary to their classifications
they are all sedatives--and they are right! I have researched the evidence and
have published my results for all both the last (click on above links). My
very strong academic background
in science and philosophy, 40 years of studies in medicine, and 12 years of building this website has driven me to investigate
the junk science and making this, as of 2009, the theme of healthfully.org. Exposing the bad promotes healthful alternatives. My investigation on the leading cause of death and disability has led me set down what I would do in case
I had CVD, and/or an AMI.
3) Essentials: There
are two common types of heart attacks, one caused by arrhythmia (irregular heart beat), for which little can be done if acute
unless in a hospital. Arrhythmia is quite common, even among children; and they
often go unnoticed. “Many
types of arrhythmia have no symptoms. When symptoms are present these may include palpitations or feeling a pause between heartbeats. More seriously there may be lightheadedness, passing out, shortness of breath, or chest pain“ Wiki. Rarely does arrhythmia result in sudden
cardiac death. Most sudden cardiac deaths that occur on the street are a result
of arrhythmia. A large subset of these deaths results from damage to the heart
muscles (thrombosis, ischemic event) from lack of oxygen; it causes the arrhythmia.
The thrombosis, when significant, result in what is called an MI, myocardial infarction, and AMI
with “A” for acute. Damage to the heart muscle in these cases can cause the heart to
beat irregularly. Nearly all AMIs
consists of two events: first the leaking of young-immature plaque (remember this)
from within the coronary artery. This leaked plaque partially restricts the blood
flow, and this then causes platelets to aggregate around the leaked plaque to form a clot (called a thrombosis). Depending
on the degree of blockage heart muscle tissue will die within the first 60 minutes from lack of oxygen (remember this). Often this will produce symptoms of an AMI. “Chest pain is the most common symptom of acute myocardial infarction and is often described
as a sensation of tightness, pressure, or squeezing…. Pain radiates most often to the left arm, but may also radiate to the lower jaw, neck, right arm, back, and epigastrium [upper-middle abdomen], shortness
of breath (dyspnea) occurs when the damage to the heart limits the output of the left ventricle, causing left ventricular failure and consequent pulmonary edema [fluid in the lungs].
Other symptoms include diaphoresis (sweating), weakness, light-headedness, nausea, vomiting, and palpitations and sudden death (frequently due to ventricular fibrillation[arrhythmia]) can occur in myocardial
infarctions. Women report more numerous symptoms
compared with men (2.6 on average vs. 1.8 symptoms in men)” Wiki. The plaque forms in the inner layer
of the artery wall, like a boil under the skin. About half of all AMIs occurs
without the signs of CVD, thus with normal level of cholesterol and no hypertension (remember this). This is because we are all forming young-immature plaque, not just those with CVD. Most of those with CVD
are forming the plaque at significantly higher rate, thus their risk is greater. The
typical young atheroma (plaque formation) causes 20% artery occlusion (remember this).
Immature plaque thus does not cause symptoms. Hypertension develops when with
advanced atherosclerosis (AS): the diameter of the arteries is reduced often by
over 50%, and the mature plaque causes the arteries to loose elasticity. Thus
the heart must pump harder to get sufficient blood to the organs and muscles, which raises the resting blood pressure. Hypertension is not the problem, just a sign of AS
and CVD. To treat hypertension is
like treating fever instead of the bacteria that causes bronchitis, it doesn’t reverse AS or prevent the formation of more young soft plaque that causes the MIs. But pharma makes billions treating the sign of AS,
hypertension. And it gets worse: a
chorus of scientist point out that cholesterol and saturated fats are not causes of
CVD & MI (except by pharma’s tobacco science), yet pharma lowers
the essential cholesterol
(link gives its long list of essential functions) with drugs and thereby harms the patients. The food manufacturers profits from the Western high-carb
(thus low fat) diet; and pharma profits from the resulting obesity-diabetes pandemic and its comorbidities. Still worse: cardiologists invasively treat mature plaque
in the coronary arteries with angioplasty and bypass surgery (see #17-28). Young plaque doesn’t show up during an angiogram (invasive imaging involving
a tube entering a major artery and going into up to 3 coronary artery where a dye is injected and x-rays are made.) Only mature plaque which results in occlusions greater than 50% shows up on an angiogram, not the
immature plaque which causes very little restrict of blood/dye flow (remember this). Mature plaque has fibrous core and hard cap,
and thus doesn’t leak to cause an AMI
(remember this). AMI is caused by the young-immature plaque (stated above). Mature plaque is
the main cause of angina pain in those who haven’t had an AMI because it
limits the flow of blood to the heart muscles, and the lack of oxygen can cause pain.
Since only mature plaque shows up on imaging (angiogram), the cardiologist treats this plaque with angioplasty and
bypass surgery; thus this procedure only reduces angina pain, it doesn’t
prevent MIs in the real-world population.
What they don’t see, they don’t treat. These invasive procedures
don’t remove the immature plaque which causes AMIs; however, pharma profits
greatly from these invasive treatments, since most of these patients will now take all the drugs their cardiologist prescribes
(averaging 6, and if patented costing about $100,000 yearly). This explains why
these invasive procedures in quality studies don’t reduce the risk of a
future MI. The small benefit gained by reducing occlusion with angioplasty is
lost because of the damage done in those procedures (see long version). The theory of lives being saved by opening or removing clogged coronary arteries is
shot down by the fact that it is the fresh small plaque that causes the AMIs. There
are over 1.5 million procedures in the U.S. annually; and those procedures aren’t worth their side effects. You now have some idea on how bad it is; the documentary videos and university lectures
and the quotes
drive this point home. I am not fooled by the cardiologist’s sophisticated
testing, complex terminology, and his faith; he is following junk clinical treatment guidelines
generated by pharma’s KOLs and reinforced by clinical quotas.
Of those who undergo imaging (angiogram), 75% of them will have occlusion
over 50% and thus likely have subsequent treatments (drugs, angioplasty, and bypass surgery). Because these subsequent treatments are not life extending or reduce the risk of AMI, I would not agree
to an angiogram.
|
|
4)
The drug miracles fare no better: Notice,
the above section didn’t mention bad cholesterol and artery clogging saturated
fats; that is because they are not
causal—for more click on
links. As for hypertension, it is a sign of
atherosclerosis not a cause. Thus
treating a sign is like treating acid indigestion with protein pump inhibitors rather
than the H. pylori bacteria which compromises the mucus lining that protects
the tissue from stomach acid. Pharma profits
much more from treating long-term chronic illnesses, rather than curing the
cause. Not surprising, lowering blood
pressure and cholesterol does not in quality studies significantly save lives
or prevent MIs. But this doesn’t
stop pharma from marketing
miracles based on tobacco type clinical trials.
Doing something isn’t the same as doing the right things; see #10 below
which lists what I do.
5) The real not so modern miracles: Let me
give you a little more about the history, and how pharma takes credit what they
haven’t accomplished. If I had the
cardiologist ear long enough, I would point out to him the three major causes
for the increase in survival. One
belatedly[1]
was the prompt and continued use of anticoagulants as not part of standard
treatment; it occurred around 1990.
Studies showed the benefit of long-term use of 325 mgs of aspirin cut
the risk of a heart attack in half. Pharma,
of course replaced aspirin with patented drugs and lowered its dose to 85 mgs;
thus at one year over 90% have developed a tolerance. Second
was the use of defibrillators and similar
methods for those with life-threatening arrhythmia and cardiac arrest. Most
significant was the decreased in smoking from 46% in 1968 to 16% in 2015. The
average smoker at 10 years had doubled
his risk of an AMI. Adding the
AMIs attributed to second-hand smoke, the rate of AMI and CVD was reduced by about 30%.
Moreover, because of fewer smokers, there were far smaller percentage of
patient with extreme CVD, thus not only
more survived but their risk of subsequent heart attacks was far less. Let
me give you two case histories to
illustrate the point. One is my father’s
experiences. He had a major heart attack
in 1953 and another in 1955, before all of the modern treatments. Both nearly
killed him, and left him with
very severe angina. He had minor heart
attacks in 1959 and another in 1962. By
1963 his angina pain was gone. He lived
23 years from his first heart attack and died in 1976 of a stroke at the age of
76. With his 1955 heart attack he stayed
in the same hospital as President Eisenhower that year. Both men had smoked
over a pack of cigarettes
a day, and then quit in the hospital.
Eisenhower died from his seventh heart attacks in 1969 at the age of
79. If they had taken subsequently to
their first AMI then standard 500 mg aspirin, they probably would have avoided
some or all of their subsequent heart attacks.
Aspirin and other anticoagulants, along with the reduction in smoking
and defibrillation, have increased survival; not the current treatments of
drugs, balloon angioplasty, stenting, and bypass surgery. Unlike the cardiologist,
I have studied how
pharma works the system and then examined the evidence for bias. I have joined
the chorus of critics. And like the critics I have uncovered a
better path to health (see #8).
6) At first sign of an MI:
I
would take sublingually (under tongue for quick absorption) a 325 mg uncoated
aspirin and 3 more with water. I carry
in my car a small pill container with 20 aspirin. This
use of aspirin is the most important of all possible treatments. Remember
(as stated above), that two events
cause an AMI, leaking young plaque
and the formation of a blood clot (thrombosis); they block the coronary
artery. The clock is running for by 60
minutes most of the damage to heart muscle has occurred, and by 90 minutes only
about 5% will benefit from treatment that
restores blood flow (the same for strokes).[2] Dead tissue cannot be brought back to
life. From time of first symptoms, only
one in 125 patients can be treated within the 90 minute window of time at 2000. Thus
the common treatment of using a clot busting drug (thrombolysis) or the
invasive balloon angiography is clearly not worth their significant risks
(including strokes, hemorrhaging, etc. (see
#16-28).
This is why it is very important for me to start with large dose of
aspirin at first sign. The antiplatelet
effect of aspirin can cause the thrombus to dissolve and prevent additional
clotting. Aspirin at a high dose (325
mg) permanently blocks the action of platelets thus prevent the clot. The body
also can come to the rescue: “In
greater than 80%
of MI the leaked plaque constitutes
less than 40% of the obstruction. Spontaneous
thrombolysis [natural
dissolving of the clot that caused the MI] occurs in about 2/3 patients within
24 hours” (Merck Manual 2006, p.
636). A review placed it at 50% from 12
to 24 hours, at
1985. I still need
to get
promptly; remember that most death occur due to arrhythmia brought on by damage
to the heart muscle. In the hospital
they have devices that can for some the patients successfully stop major left
ventricle arrhythmia and resuscitate from cardia arrest. However, I wouldn’t
take their drugs that are
supposed to reduce the chances of arrhythmia.
These drugs are not magic bullets that target the heart’s vagus nerve, they would affect both my cognitive function and weaken the
beating of my heart (both bad things).
Getting promptly to the hospital could save my life.
7) Take
charge: knowing the role of pharma,
I would inform the cardiologist that it is my body; I will decide what you do
to it. I would not take a sedative,
being drugged the cardiologist would make my treatment choices. Sedatives
are given many names including
anti-nausea, muscle relaxant, mood elevator, analgesic (pain) to name some. Also on my do not take list are drugs for high
blood pressure (they too weaken the heart muscle) and affect cognitive
function. For one thing hypertension is
not the problem, so why treat it? Every
additional drug multiplies the risk of an adverse reaction/interaction. Secondly
the widely prescribed ace inhibitors
and beta blockers are sedatives that block the catechol-amine
neurotransmitters. This causes the
relaxation of the smooth muscles that make up the artery walls and also those
that make the heart beat. This affect
upon the heart increase the risk for heart failure (heart failure occurs when
the heart muscle is too weak to pump sufficient blood). In general, if among
side effects for a drug
are dizziness and drowsiness it has sedative properties, which includes though
often not listed reduced cognitive function.
How much depends upon dose. Some
of them are subtle because they gradually build up in the adipose tissue. Even
the antihistamines function also as
sedatives. I need to be alert and have
good muscle tone so that I can cognitively will my heart to beat stronger. Since
I have already taken over 2 grams of
aspirin, I would refuse their anticoagulants—more is not better because of the
risk of hemorrhaging. They are at this
point not needed since the aspirin has been shown to be extremely
effective. If the pain is significant I
would take an opiate preferable morphine; it has been standard treatment for
over 70 years. If given an IV,
lidocaine—it has been used for over 40 years--moderately reduces the risk of
arrhythmia as does opiates. Arrhythmia
drugs are quite risky since they have been proven to cause when taken long-term
heart failure. Short-term there is no
major benefit. The IV can increase my
blood pressure if below 60, and can be used to administer adrenalin and noradrenaline
(epinephrine and norepinephrine), which are powerful heart stimulants. They
can prevent heart failure.[3] Other life-saving interventions include CPR
(cardio-pulmonary resuscitation),
defibrillation, cardioversion (both are electric shock to chest which can alter
arrhythmia), and a pacemaker to prevent major arrhythmia. But I would let the
cardiologist take charge, because of pharma’s role in treatment
guidelines. The body has evolved
mechanism to deal with crisis; I have faith in those mechanisms.
8)
Razzle-dazzle
experts educated by pharma: Testing
is part of the razzle-dazzle used to gain my confidence in the cardiologist who
wishes to take charge and follow pharma’s treatment guidelines and to meet
their clinic’s business quotas. As state
in 3), I would avoid the angiogram (invasive imaging) since it does not lead to
beneficial treatments and it has major risks (see long
#18)[4]. There is no purpose in knowing where the
coronary artery is blocked since that knowledge doesn’t lead to a positive
treatment. In paragraph 2, I explained
why I believe that an angiogram (invasive imaging) leads to angioplasty, and it
is not life extending. Quality studies
show that (balloon angioplasty or insertion of stent) when administered after
the first 90 minutes from first symptoms
doesn’t reverse the damage to the heart muscle.
What the cardiologist believes is not supported by the evidence, evidence
which he probably hasn’t heard of in his CME
classes given by pharma’s KOLs.
Sincerity and experience doesn’t replace the
evidence from quality clinical trials.
I would submit to an angiogram, the gateway to stenting and bypass
surgery. Doctors sell the fluff.
[1]
Belatedly since powerful anticoagulants were used from the late 40s for the
first 2 to 4 weeks following an AMI.
[2] Based on pharma’s tobacco studies, guidelines
have extended the window to 3 hours. The
5% is questionable since with pharma involvement through KOLs, all trials and
studies are biased. The reviewers for
the journal do not see the raw data. A
study where the raw data was made available through FIOA found in 74 published
articles 32% average (between11-69%)—NEJB
2008.
[3] They are 2 of the catechol amines which beta
blockers inhibit.
[4] I shudder when I visualize a hard-long object
being pushed through my arteries from my leg into my heart. I can see it bumping-rubbing
against
(damaging) the paper-thin single layer of endothelial
cells that have essential
functions as a barrier and regulator.
4)
The drug miracles fare no better: Notice, the above section didn’t mention
bad cholesterol and artery clogging saturated fats; that is because they are not causal—for
more click on links. As for hypertension,
it is a sign of atherosclerosis not a cause. Thus treating a sign is like treating
acid indigestion with protein pump inhibitors rather than the H. pylori bacteria which compromises the mucus lining that protects
the tissue from stomach acid. Pharma profits much more from treating long-term
chronic illnesses, rather than curing the cause. Not surprising, lowering blood
pressure and cholesterol does not in quality studies significantly save lives or prevent MIs.
But this doesn’t stop pharma from marketing miracles based on tobacco
type clinical trials. Doing something isn’t the same as doing the right
things; see #10 below which lists what I do.
5) The real not so modern miracles: Let me give you a little more about the history,
and how pharma takes credit what they haven’t accomplished. If I had the
cardiologist ear long enough, I would point out to him the three major causes for the increase in survival. One belatedly was the prompt and continued use of anticoagulants as not part of standard treatment; it occurred around
1990. Studies showed the benefit of long-term use of 325 mgs of aspirin cut the
risk of a heart attack in half. Pharma, of course replaced aspirin with patented drugs and lowered its dose to 85
mgs; thus at one year over 90% have developed a tolerance. Second
was the use of defibrillators and similar methods for those with life-threatening arrhythmia and cardiac arrest. Most significant was the decreased in smoking from
46% in 1968 to 16% in 2015. The average smoker at 10 years had doubled his risk
of an AMI. Adding the AMIs attributed to second-hand smoke, the rate of AMI and CVD was reduced by about 30%. Moreover, because of fewer smokers,
there were far smaller percentage of patient with extreme CVD, thus not only more
survived but their risk of subsequent heart attacks was far less. Let me
give you two case histories to illustrate the point. One is my father’s
experiences. He had a major heart attack in 1953 and another in 1955, before
all of the modern treatments. Both nearly killed him, and left him with very
severe angina. He had minor heart attacks in 1959 and another in 1962. By 1963 his angina pain was gone. He lived 23 years from his
first heart attack and died in 1976 of a stroke at the age of 76. With his 1955
heart attack he stayed in the same hospital as President Eisenhower that year. Both
men had smoked over a pack of cigarettes a day, and then quit in the hospital. Eisenhower
died from his seventh heart attacks in 1969 at the age of 79. If they had taken
subsequently to their first AMI then standard 500 mg aspirin, they probably would have avoided some or all of their subsequent
heart attacks. Aspirin and other anticoagulants, along with the reduction in
smoking and defibrillation, have increased survival; not the current treatments of drugs, balloon angioplasty, stenting, and
bypass surgery. Unlike the cardiologist, I have studied how pharma works the
system and then examined the evidence for bias. I have joined the chorus of critics. And like the critics I have uncovered a better path to health (see #8).
6) At first sign of an MI:
I would take sublingually (under tongue for quick absorption) a 325 mg uncoated aspirin and 3
more with water. I carry in my car a small pill container with 20 aspirin. This use of aspirin is the most important
of all possible treatments. The same approach I would follow if having a
stroke. Remember (as stated above), that two
events cause an AMI, leaking young plaque and the formation of a blood clot (thrombosis);
they block the coronary artery. The clock is running for by 60 minutes most of
the damage to heart muscle has occurred, and by 90 minutes only about 5% will
benefit from treatment that restores blood flow (the same for strokes). Dead tissue cannot be brought back to life. From time of first symptoms, only one in 125 patients can be treated within the 90 minute window of time
at 2000. Thus the common treatment of using a clot busting drug (thrombolysis) or the invasive
balloon angiography is clearly not worth their significant risks (including strokes, hemorrhaging, etc. (see #16-28). This is why it is very important for me to start with large dose
of aspirin at first sign. The antiplatelet effect of aspirin can cause the thrombus
to dissolve and prevent additional clotting. Aspirin at a high dose (325
mg) permanently blocks the action of platelets thus prevent the clot. The body
also can come to the rescue: “In greater than 80% of MI the leaked plaque constitutes less than
40% of the obstruction. Spontaneous thrombolysis
[natural dissolving of the clot that caused the MI] occurs in about 2/3 patients within
24 hours” (Merck Manual 2006, p. 636). A review placed it at 50% from
12 to 24 hours, at 1985. I still need to get
promptly; remember that most death occur due to arrhythmia brought on by damage to the heart muscle. In the hospital they have devices that can for some the patients successfully stop major left ventricle
arrhythmia and resuscitate from cardia arrest. However, I wouldn’t take
their drugs that are supposed to reduce the chances of arrhythmia. These drugs
are not magic bullets that target the heart’s vagus nerve, they would affect both my cognitive function and weaken the beating
of my heart (both bad things). Getting promptly to the hospital could save my
life.
7) Take charge: knowing the role of pharma, I would inform the cardiologist that
it is my body; I will decide what you do to it. I would not take a sedative,
being drugged the cardiologist would make my treatment choices. Sedatives
are given many names including anti-nausea, muscle relaxant, mood elevator, analgesic
(pain) to name some. Also on my do not take list are drugs for high blood
pressure (they too weaken the heart muscle) and affect cognitive function. For
one thing hypertension is not the problem, so why treat it? Every additional
drug multiplies the risk of an adverse reaction/interaction. Secondly the widely
prescribed ace inhibitors and beta blockers are sedatives that block the catechol-amine neurotransmitters. This causes the relaxation of the smooth muscles that make up the artery walls and also those that
make the heart beat. This affect upon the heart increase the risk for heart failure
(heart failure occurs when the heart muscle is too weak to pump sufficient blood). In
general, if among side effects for a drug are dizziness and drowsiness it has sedative properties, which includes though often
not listed reduced cognitive function. How much depends upon dose. Some of them are subtle because they gradually build up in the adipose tissue. Even the antihistamines function also as sedatives. I need
to be alert and have good muscle tone so that I can cognitively will my heart to beat stronger. Since I have already taken over 2 grams of aspirin, I would refuse their anticoagulants—more
is not better because of the risk of hemorrhaging. They are at this point not
needed since the aspirin has been shown to be extremely effective. If the pain
is significant I would take an opiate preferable morphine; it has been standard treatment for over 70 years. If given an IV, lidocaine—it has been used for over 40 years--moderately reduces the risk of arrhythmia
as does opiates. Arrhythmia drugs are quite risky since they have been
proven to cause when taken long-term heart failure. Short-term there is no major
benefit. The IV can increase my blood pressure if below 60, and can be used to
administer adrenalin and noradrenaline (epinephrine and norepinephrine), which are powerful heart stimulants. They can prevent heart failure. Other life-saving interventions include CPR
(cardio-pulmonary resuscitation), defibrillation, cardioversion (both are electric shock to chest which can alter arrhythmia),
and a pacemaker to prevent major arrhythmia. But I would let the cardiologist take charge, because of pharma’s role in treatment guidelines. The body has evolved mechanism to deal with crisis; I have faith in those mechanisms.
8)
Razzle-dazzle experts educated by pharma: Testing is part of the razzle-dazzle used to gain my confidence in the cardiologist who wishes to take
charge and follow pharma’s treatment guidelines and to meet their clinic’s business quotas. As state in 3), I would avoid the angiogram (invasive imaging) since it does not lead to beneficial treatments
and it has major risks (see long #18). There is no purpose in knowing where the coronary artery
is blocked since that knowledge doesn’t lead to a positive treatment. In
paragraph 2, I explained why I believe that an angiogram (invasive imaging) leads to angioplasty, and it is not life extending. Quality studies show that (balloon angioplasty or insertion of stent) when administered
after the first 90 minutes from first symptoms doesn’t reverse the damage
to the heart muscle. What the cardiologist believes is not supported by the evidence,
evidence which he probably hasn’t heard of in his CME classes given by pharma’s
KOLs. Sincerity and experience doesn’t
replace the evidence from quality clinical trials. I would submit to an
angiogram, the gateway to stenting and bypass surgery. Doctors sell the fluff.
9) Why pharma is against aspirin: long-term daily aspirin 325 mg dose (not the baby aspirin) reduces the risk of most cancers
(if not all) over 35%, and also the risk of the cancer becoming metastatic. One
mechanism is that it promotes the death of abnormal cells through the body’s necrosis factor. Also the 325 mg slows the progression of atherosclerosis
which causes CVD and thus its assorted signs including hypertension. Aspirin prevent heart attacks and pulmonary embolisms by preventing blood clots, thus it competes with
their anticoagulants. So doctor’s recommend the baby aspirin for which
tolerance quickly develops. Aspirin competes with drugs for migraine head ache,
and drugs for moderate pain. And until the 1980s it was the most widely used
drug to treat arthritis. It also lowers the risk of Alzheimer’s disease. Regular usage of the other drugs in the NSAID family, including acetaminophen,
through inhibition of COX-2, they increase the risk of heart attacks, but not aspirin which affect a different pathway--see. To limit aspirin’s market presence doctors are repeatedly
warned about the risk of an ulcer and that children shouldn’t take it because of Reye syndrome(which
happens to be the extremely rare)—more pharma’s tobacco ethics and tobacco science. Moreover it costs a penny a day. Aspirin is natural; the salicylic
acid form is widely produced by plants. Mammals, like with vitamins, has evolved
mechanisms for usage. Pharma is in the business of marketing drugs for illnesses,
thus pharma is against aspirin.
I have been taking a 325 mg or two daily since 1992.
10). Positive
things to do: I would upon release
from the hospital resume exercising, continue use of aspirin
apply a high dose of testosterone
lotion from a compounding pharmacy to promote heart muscle healing, and I would take antioxidants CoQ10
and vitamin C
1000 mg each to reduce damage from reactive oxygen species (ROS)
to prevent endothelial damage
to the artery walls. I would also not
eat a Western diet
which is very high in sugar (fructose is the problem)
and refined carbs. The diet high in fructose from table sugar and glucose from
starches and table sugar is the basic cause for the global diabetes and obesity pandemics.
If I had a weight problem I would go on a ketogenic diet
to cleanse my liver of excess fat caused by the conversion of fructose to fat in the liver where it is stored. Diet related articles are found at link. The video library
will wash away all doubts. “To every problem there is a short answer, and
it is wrong”, H.L. Mencken.
^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^
1) Intro on bad pharma
2) Revolt among doctors.
3) Essentials: dead tissue, leaking and firm plaque, angioplasty
& CABG
4) Drugs not so modern miracles
5) The not so modern miracles
6) At first sign of an MI: aspirin and promptly go to hospital
7) Take charge
8) Razzle-dazzle, taking charge;
no to sedatives, hypertension drugs, anticoagulants,
9) Why pharma is against aspirin
Positive things to do
| This is stable plaque, encapsulated |

|
| The expansion of artery is loss when cut |
A photo of
atherosclerotic plaque of a carotid artery.
“The atheroma (accumulation and swelling in an artery wall) in the
carotid artery consisting of lipids (cholesterol and fatty acids), calcium,
fibrous connective tissues, and macrophage cells (large white cells that among
other things engulf and then digest cellular debris and pathogens, stimulate
lymphocytes and other immune cells, and function to stimulate the regeneration
of tissue). While in the early stages, based on gross
appearance, have traditionally been termed fatty
streaks by pathologists, they are not composed of fat
cells, i.e. adipose
cells, but
of accumulations of white
blood cells, especially macrophages, that have taken up oxidized low-density
lipoprotein (LDL). After
they accumulate large amounts of cytoplasmic membranes (with associated high
cholesterol content) the macrophages are called foam
cells. When
foam cells die, their contents are released, which attracts more
macrophages and creates an extracellular lipid core near the center to inner
surface of each atherosclerotic plaque.
With aging, the outer,
older portions of the plaque become more calcified, less metabolically active
and more physically stiff over time.
Younger plaque can break off and cause a blockage downstream, the major
cause of heart attacks and strokes. It
can also affect other organs such as the kidney. Older plaque is stable and
unlikely to cause
a medical emergency, though, for example, it can cause stable angina. Most
MIs occur with less than 50% stenosis (narrowing) and typically at
locations with about 20% stenosis (narrowing), prior to sudden lumen closure
and resulting myocardial infarction (see footnote for treatment implications of
this fact)” Wiki (with
editing by jk to improve comprehension by
a wider audience).
Atheroma and
changes in the artery wall usually
result in small aneurysms (enlargements) just large enough to compensate for the extra wall
thickness with no
change in the lumen diameter. However, eventually, typically as a result of
rupture of (unstable) vulnerable
plaques and clots within the lumen over the plaque, stenosis (narrowing) of the vessel develops in some areas.
Less frequently, the artery enlarges so much that a gross aneurysmal enlargement of the artery results. All three
results are often observed, at different locations, within the same
individual. Over time, atheromata usually progress in size
and thickness and induce the surrounding muscular central region (the media) of
the artery to
stretch out, termed remodeling, typically just enough to compensate for their
size such that the caliber of the artery opening (lumen) remains unchanged
until typically over 50% of the artery wall cross-sectional area consists of
atheromatous tissue. If a rupture occurs of the endothelium and
fibrous cap, then a platelet and clotting response over the rupture rapidly
develops. Additionally, the rupture may result in a shower of debris. Platelet and clot accumulation
over the rupture may produce narrowing/closure of the lumen, and tissue damage
may occur due to either closure of the lumen resulting in loss of blood flow
beyond the ruptured atheroma and/or by occlusion of smaller downstream vessels
by debris. This is the principal mechanism of myocardial
infarction, stroke or
other related cardiovascular
disease problems. As
stated above most MIs result from rupture of unstable plaques and such plaque
normally accounts causes under 20% occlusion.
^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^ Non-technical Summation
Heart
Attacks (MI) and treatments:
“Each year [2005] 1.5 million Americans experience a heart attack
and nearly 460,000 are fatal. Of
those
who die, almost half die suddenly, before they can get to a hospital” AHA. As with most acute conditions the list of
standard treatments, most are not worth the side effects.
Following the list below when the patient is
depending upon the help requires making the doctor aware of who is the ultimate
decider. With MI, there are two
phases
acute and recovery. What works: Because tissue dies quickly, depending on
the degree of blockage, the PCI is modestly superior to the thrombolysis (balloon
angioplasty compared to clot-busting drug).
The main benefit is within 90 minutes of first symptoms. After 3 hours neither procedure is worth the
risks and side effects (as with all things medical the benefits are greatly
oversold and the risks understated). For
arrhythmia there are drugs not worth taking, and physical interventions should
be permitted only in the most serious of circumstance. The drug best interventions are nitroglycerine
for angina pain and improved circulation, morphine for pain and sedation,
lidocaine for arrhythmia, epinephrine (adrenalin), and aspirin in high dose, up
to 2.5 grams per day as blood antiplatelet effect and anti-inflammatory.
All of these things have been attacked by
pharma using junk science trials and fed to doctors through pharma’s thought
leaders (see). For recovery the
typical
well insured patient is treated long-term for a variety of issues that cost on
an average over $100,000 per year.
Nearly all of them have better alternatives.
CRITICAL
CARE AVOID: (in order of importance):
downers (psychotropic drug), Protein Pump Inhibitor (PPI), heparin
& other blood
thinners, high blood pressure medication
except if extreme 180 over 110, antiarrhythmics
except for lidocaine, and oxygen. Downers (psychotropic drugs) have many
indications such as anti-nauseas, muscle relaxant, sedative. If drowsiness or
mental confusion is a side effect, it is probably a downer (or an opiate).
Some have been approved for
hypertension. Drugged, the patient
is
less likely to inform the nurse of a negative turn in their condition, or
resist their doctor’s advice. PPIs
for
acid indigestion are addicting. Instead
of heparin or similar anticoagulant promptly take 975 mgs aspirin, followed by
one every 4 hours. Drugs for
hypertension other than nitroglycerin do not lower morality Cochrane
Library and many of them
are
downers. RECOVERY AVOID: PPI is given
with the anticoagulant,
but PPIs are addicting because of the rebound effect, and long-term usage
causes serious life-shortening, side effects such as osteoporosis &
colitis. Tums, when needed, is a
better
choice. Statins are totally over sold,
and are justified only by marketing
science. Counter
to their marketing
science, they are not cardiovascular protective through they improved the lipid
profile and thus are not worth the side effects. PPI,
statin, blood pressure drugs, blood thinner, antiarrhythmics drug therapy, and
downer lack quality evidence that proves their
net worth and superiority to other choices; yet
they are routinely administered in the hospital and nursing home, when the
patient is most vulnerable. Avoid polypharmacy because it multiplies the risk of major side effects. All too often their side effects are treated
with additional drugs. All side
effects are grossly under-reported. Most drugs started in the hospital and
nursing home will be continued long-term.
While recovering, avoid both stent and
bypass operation, they do not prolong significantly life, though they
reduce angina pain. “The vast majority of MIs do not originate with obstructions that
narrow arteries" Wiki. Coronary heart disease
is caused by
atherosclerosis, with the young, unstable plaque causing over 80% of the
myocardial farctions. This results
from
damage to LDL in the artery wall which elicits an immune response.
Thus high level of cholesterol and
hypertension are a result of atherogenesis.
Thus the best long-term way to prevent subsequent MI is to prevent
damage to LDL and lower the immune response.
This is effectively accomplished by taking 300 mg of CoQ10 and 325 mg of aspirin with each meal.
The natural estradiol 2mg lowers the risk for
women of MI by 50%, and testosterone should be taken sufficient dose to raise
the serum level to above 500 ng/dL. Aspirin
anti-inflammatory effect prevents at the high dose atherogenesis, while at 325
mg per day lowers risk of blood clots. CoQ10
is the best of antioxidants. Unfortunately
the physician is not a reliable
source of information, his continuing
education classes are given by pharma; a pharma that does marketing studies
to convince through their opinion leaders that these off-patent drugs are
ineffective and dangerous.
|
