|
Pharmaceutical industry data
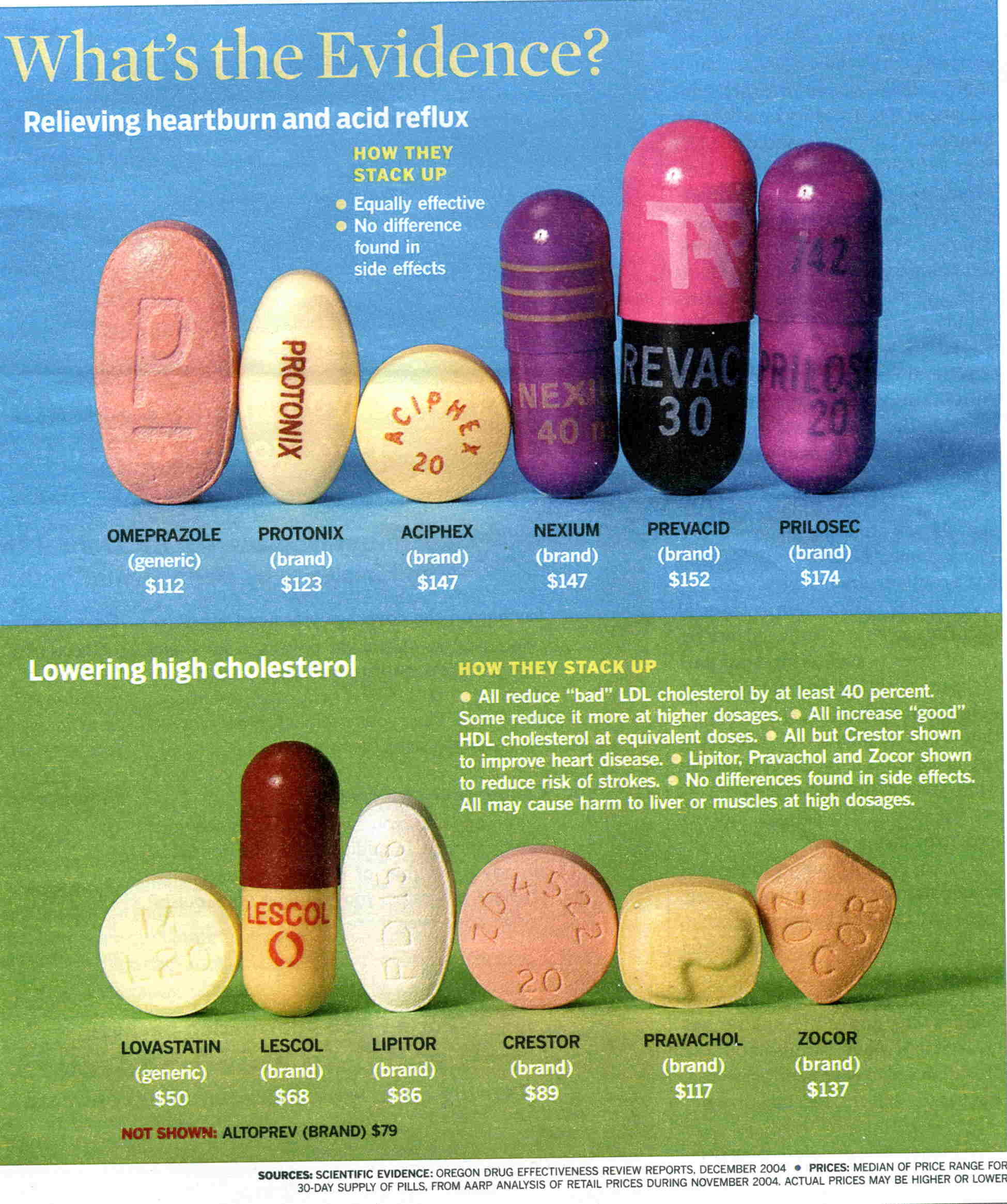
Scientific Evidence: Oregon Drug Effectiveness Review Report, December 2004. Prices: Median of price range for 30-day supply of pills from AARP analysis of retail prices
during November 2004. [For scanned picture]
New medicines 1975 to 1997 licensed world wide was 1,223 of which only 4 were developed by the pharmaceutical
industry R&D activities—source Journal of the American Medical Association
Indian, one of the few developing countries which has a pharmaceutical industry spends only 2% of its revenue
on R&D ($152 million), while the major pharmaceutical companies spend 15.6 ($33.2 billion)—source Organization
of Pharmaceutical Producers of India.
Cost per year of saving a life by
malaria vaccine $15; through chemotherapy for breast cancer $58,000.
The market for pharmaceuticals in low-income countries is small.
|
CONTINENT |
DISEASE BURDEN |
REVENUES |
|
Americas |
9.77% |
76.3% |
|
Europe & Middle East |
19.42% |
15.37% |
|
Asia - Pacific |
46.4% |
5.68% |
|
Africa |
24.25% |
0.29% |
Sources: Pharmaceutical Manufactures Association 2004; World Health Organization 2004
Disease burden as cause of death:
33% in poor countries, 2.5% in rich countries.
|
CAUSE |
DEATHS/DAY
POOR COUNTRIES |
DEATHS/DAY
RICH COUNTRIES |
|
Lower respiratory infections |
7830 |
923 |
|
HIV |
5861 |
56 |
|
Diarrheal disease |
4210 |
16 |
|
Malaria |
3409 |
1 |
|
Tuberculosis |
3000 |
41 |
Source: WHO Global Burden of Disease, 2004 project
http://healthyskepticism.org/, The Medical Lobby for Appropriate Marketing (MaLAM) was established
in 1983 and in 2001 changed to a new name: Healthy Skepticism. An excellent resource
for articles both from journal and the popular press.
Healthy
Skepticism Library number: 1785
Publication type: journal article
Ismail A.
Prescription for Power: Drug makers'
lobbying army ensures their legislative dominance
The Center for Public Integrity 2005 Apr 28
Full text:
The
deep-pocketed pharmaceutical and health products industry has lobbied on more than 1,400 congressional bills since 1998 and
spent a whopping $759 million during that period, a Center for Public Integrity review of lobbying records revealed. Drug
companies and manufacturers of health products have used more professional lobbyists in the last six and a half years—almost
3,000—than any other organized interest, the analysis also found. In comparison, the insurance industry, second-largest
in terms of spending, spent $644 million in the same period and employed just over 2,000 lobbyists.
In recent years,
the pharmaceutical industry has scored a series of legislative victories on Capitol Hill, which could potentially translate
into tens of billions of dollars of additional revenue to drug companies annually. The federal government will buy drugs worth
at least $40 billion from the companies every year once the Medicare Prescription Drug, Improvement, and Modernization Act
of 2003 goes into effect next year. In addition, critics have accused the industry of having undue influence over the Food
and Drug Administration, the agency that regulates pharmaceutical interests.
For every member of Congress in office
since '98, there were four and a half pharmaceutical industry lobbyists.
Industry-watchers say the drug companies'
recent successes in Congress and with the FDA show how effective their lobbying campaign is. "The [lobbying] money is very
well-spent," said Dr. Jerry Avorn, author of Powerful Medicines: The Benefits, Risks, and Costs of Prescription Drugs. "The
fact that we are the only country in the industrialized world that does not have any provision for negotiating drug prices,
the fact that we are spending far more per capita on drugs than any other country and the fact that when legislation is written
it often seems to be exactly the kind of legislation that benefits the pharmaceutical industry [shows] they are getting their
money's worth."
Find out more about the pharmaceutical and health products industry's lobbying
In 2003,
the year that the legislation passed allowing prescription drug coverage through Medicare, 298 pharmaceutical and health industry
groups spent $143 million lobbying the federal government. They employed 1,274 professional lobbyists.
The passage
of the new Medicare law had been an industry priority for many years. No wonder: The 415-page legislation contains several
windfalls for drug companies, including a controversial provision that prohibits the federal government from negotiating with
companies on drug prices.
The industry has also mounted campaigns to weaken federal regulation, strengthen patent
protections, extend patents, win tax credits and get the federal machinery to protect its interests abroad, among other issues.
Other big wins on Capitol Hill include the extension of the Prescription Drug User Fee Act through September 2007,
authorizing the FDA to continue collecting industry money to process drug approval applications. The FDA expects to take in
more than $284 million in user fees this year alone. The user fee has helped FDA to hire more than 1,200 new employees—and
thereby to reduce drug approval time. But many observers, such as Avorn and Thomas Moore, a fellow at George Washington University's
Center for Health Services Research and Policy and author of Prescription for Disaster, a book on drug safety, oppose the
arrangement because that money gives the industry greater leverage. The user fee act implies that the main mission of the
FDA is to facilitate speedy approval of drug, Avorn said. He added that the legislation and the agency's "shrinking capacity
to follow post-marketing safety problems, all together suggest that the needs of the industry have loomed larger at FDA than
public health mission."
"The User Fee Act has left the pharmaceutical industry paying a very significant share of
FDA's total budget," Moore said. "Each reauthorization is sort of another step to come to the bargaining table, if you will,
to see if they can obtain some additional benefits."
Many critics also argue that by making the FDA dependent on the
industry, it also opens the doors for a culture of conflict-of-interest to thrive.
In 2002, the industry also succeeded
in getting the Best Pharmaceuticals for Children Act passed. The law encourages companies to test drugs in kids by extending
patents for six months.
Drug interests have also successfully blocked a number of bills that would have affected its
bottom line, among them, legislative efforts to control drug prices, legalizing drug importation, closing loopholes in patent
laws etc.
Former government insiders
Leading the industry's lobbying efforts was the trade group Pharmaceutical
Research and Manufacturers of America, the seventh largest lobbying organization in the country. PhRMA alone spent almost
$93 million on lobbying in the last six and a half years.
Besides its 38 in-house lobbyists, PhRMA employed
160 lobbyists in 2003-2004. Since 1998, the organization used 64 different firms to lobby 35 federal agencies on 38 issues
separately identified under the Lobbying Disclosure Act of 1995.
The Biotechnology Industry Organization, a trade
organization that represents biotech and biomedicine companies, spent more than $27 million since '98.
The Center
analysis revealed the extent to which the industry used former government insiders to influence the federal government. Of
the nearly 3,000 professionals who lobbied for the industry, 805 were former federal officials, including more than 50 former
members from the House and a dozen from the Senate.
Both PhRMA and BIO are headed by former members of Congress. PhRMA's
president is former Rep. Billy Tauzin (R-La.), who chaired the House energy and commerce committee until last year and was
one of the co-sponsors of the Medicare legislation. The House Energy and Commerce Committee's jurisdiction includes the drug
industry. Tauzin's former colleague on the committee, James Greenwood (R-Pa.) heads BIO. The former Pennsylvania congressman,
who sponsored or backed numerous bills favorable to the industry, including the Best Pharmaceuticals for Children Act of 2002,
joined BIO last July under controversial circumstances. As chairman of the Energy and Commerce Committee's Subcommittee on
Oversight and Investigation, just before he accepted the position he was scheduled to hear testimony on possible links between
antidepressant use and suicide among children. Because of the conflict of interest, he cancelled the hearing.
Both
Tauzin and Greenwood have not yet registered to lobby—both recently retired congressmen have to wait for at least a
year before they can legally lobby their colleagues. But the industry has employed at least 48 former members of the U.S.
House of Representatives and 15 ex-senators to lobby.
That includes Sens. Bob Dole (R-Kan.), Birch Bayh (D-Ind.),
Lloyd Bentsen (D-Texas), Dennis Deconcini (D-Ariz.), Steve Symms (R-Idaho), Tim Hutchinson (R-Ark.) and Howard Baker (R-Tenn.)
and Reps. Bob Livingston (R-La.), Bill Paxon (R-N.Y.) and James Blanchard (D-Mich.). Dole and Bayh are the authors of the
Bayh-Dole Act of 1980, which gave the drug industry greater access to government-funded research.
The Center's findings
didn't surprise the industry's longtime critics. Rep. Bernie Sanders (I-Vt.), who has introduced several measures in Congress
to regulate drug companies, says that the pharmaceutical industry has the most powerful lobby in Washington, D.C.. "Uniquely
in the industrialized world, our government does not regulate the pharmaceutical industry—rather the pharmaceutical
industry regulates the government, which is why Americans pay by far the highest prices in the world for medicines they need,"
he told the Center.
The Orange County Register,
Health & Science Section, Weds., Oct. 20, 1999, p. 20.
In Drug Studies, Money Counts
FUNDING:
Drug-company sponsorship makes for less-critical views, researchers say.
By DON BABWIN
The Associated Press
CHICAGO — Studies on the cost-effectiveness of drugs are far more likely to report
favorable findings if they are sponsored by the drug companies themselves rather than independent groups, researchers
found.
Their study — funded by a pharmaceutical company — appears to confirm long-held
suspicions that doctors are less critical about a drug's safety and effectiveness when they have financial ties to the manufacturer.
"It is possible that these factors may result in some unconscious bias"
in interpreting a study's findings, the researchers said.
Last year, the conflict-of-interest issue made headlines when a report found
that the vast majority of doctors who defended the safety of calcium channel-blockers had a financial relationship with manufacturers
of the blood-pressure pills. In the current study, published in today's
Journal of the American Medical Association, the researchers looked at 44 studies on the cost-effectiveness of cancer
drugs. Twenty of the studies were funded by pharmaceutical companies and 24 by nonprofit organizations. Those
sponsored by nonprofit groups reached unfavorable conclusions 38 percent of the time, compared with just 5 percent for
studies sponsored by pharmaceutical companies. Also, researchers in company-backed studies were slightly more likely
to overstate the cost-effectiveness. Some researchers receive funding directly
from pharmaceutical companies. Some get funding in the form of honoraria or travel expenses. Some hold stock in
drug companies and profit directly from increased drug sales.
Dr. Charles Bennett, the lead author and a professor at Northwestern Medical School,
said that in addition to the possibility
of unconscious bias, there could be other explanations for the findings.
For example, pharmaceutical
companies are given early looks at studies. That enables them to abandon studies that appear to be unfavorable and focus on
those they think are going to be positive, Bennett said. Bennett said the findings
should not be seen as a major criticism of pharmaceutical companies. "Our study
was sponsored by a pharmaceutical company," he said, adding that the company, Amgen Inc., did not comment on it before
publication. He also said his paper analyzed studies sponsored by Amgen, which fared no better than other company-sponsored
studies. Bennett said the best thing would not be to stop pharmaceutical
companies fr6m sponsoring research, but to get other types of sponsors to underwrite studies, too, such as
managed-care organizations.
Amgen spokesman David Kaye said: "If you want the best physicians in the world,
you have to let them run the trials.
If you kill a study or over-control it, word gets out and the best investigators won't do your studies." Others not involved with the study said the findings raise serious concerns.
"The best hypothesis I can tell for that is the person doing the research has internalized
the values of their funder," said Sheldon Krimsky, a Tufts University professor who studies scientific integrity and
conflict of interest and who wrote an editorial about the study in JAMA. Dr.
Sidney Wolfe, director of Public Citizen's Health Research Group in Washington, agreed: "As in other studies of the drug
industry, this shows the financial interests of the drug industry rides over the actual data."
Comments on the 1992 legislation affecting the FDA, which
required the drug companies to contribute to most of the cost for the approval of new drugs and which was followed by budget
reductions of the FDA so that it couldn’t fund follow-up studies on safety and efficacy of approved drugs. These legislative
changes were lobbied for by the drug industry. The second is to further weaken
the position of the smaller companies by adding an additional expense which thereby forced them to be even more dependent
upon the drug giants in raising the funds for the trials and now also for FDA approval.
How do you get honest reliable data:
1). Have the drug companies contribute
to a research pool, much like the way the State & Federal government contribute to the universities in a state to do other
types of research. Then let the university departments and the Graduate Study
Department work out how those funds are to be allocated.
2). Drug companies could still do basic
research, but the clinical trials would be run by the universities.
3). Those drugs developed by the universities
could then manufactured at a cost plus formulation, with the profits therefrom flowing back into the general pool.
1a). Permit the university departments
to funnel research into drugs into those area where the needs are greatest, such as where there is a lack of effective treatment,
the lost to society is greater, and where it seems that an effective medication would be sufficiently likely to be produced
in relatively short period of time. They would be less likely to fund research
on a me-to type of knockoff drugs which now make up 90% of the drugs approved by the FDA.
2 & 3). This would result in a much
smaller role of the Pharmaceutical industry. The benefits of this would be lower
prices for drugs, a competitive advantage over foreign companies by lower pricing, and increased effort to develop drugs based
on needs rather than profits.
|