Is
Less More? New Study Challenges Conventional Thought on Desirable Cholesterol Levels, Links Very Low Cholesterol to Cancer
Worst Pills Best Pills Newsletter
article February, 2008
In the U.S.,
current thinking about cholesterol is generally that “lower is better.” But there is a growing body of evidence,
most recently a study published in the July 2007 Journal of the American College
of Cardiology, that suggests very low cholesterol levels are linked to cancer.
This leaves two fundamental questions unanswered: How low is low enough? And might there be dangers
from going too low?
The issue is not so cut-and-dry. High cholesterol, especially if accompanied by other risk factors, can lead to very serious cardiovascular problems
such as hardened arteries, strokes and heart attacks. And because heart disease is the leading cause of death in the U.S.
– claiming over 650,000 lives in 2004 alone, according the Centers for Disease Control and Prevention – there
has been a major push from the public health community to fight heart disease head on.
To this end, the Department of Health and Human Services, through the National Cholesterol Education
Program (NCEP), has worked since 1985 to “reduc[e] the percentage of Americans with high blood cholesterol” through
education programs aimed both at the public and health professionals. The project has been successful in achieving its goals,
dramatically increasing blood cholesterol screening and lowering average total cholesterol levels among U.S.
adults from 213 mg/dL to 203 mg/dL since 1978. In its most recent guidelines, the NCEP pushed harder for still lower cholesterol
levels, suggesting drug therapy for almost all high-risk patients with an LDL-C (“bad”
cholesterol) of 100 and over.
But how the new study fits into this traditional treatment of high cholesterol is unclear at
this point.
Study causes controversy among editors
The Journal of the American College
of Cardiology study was a metaanalysis examining the relationship between lowering LDL-C
using statins and the development of cancer.
A meta-analysis, such as the one done for this study, involves combining data from studies already
published or completed to see trends that might be missed in any one individual study. In this case, the authors limited their
data to the 13 large, randomized, controlled (with a comparison group) trials on statins published up to November 2005 that
included data on newly diagnosed cancer. Although in all these studies there was a comparison group that did not receive the
statins, those study participants were not included in the meta-analysis. The four statins that met the criteria were lovastatin (MEVACOR), simvastatin (ZOCOR), fluvastatin (LESCOL) and pravastatin (PRAVACHOL) .
In their analysis, researchers found a “highly significant inverse
relationship between achieved LDL-C levels and rates of newly diagnosed cancer.” In other words, researchers saw more new cases of cancer
in patients with the lowest cholesterol levels. However, cancer rates were not related to the degree of LDL-C
lowering – that is to say, cancer rates were not linked to how much the cholesterol levels decreased, but how low cholesterol
levels became. While it is true that the cholesterol lowering in the meta-analysis was obtained by treatment with statins,
similar cholesterol lowering by other methods (diet, exercise or other cholesterol- lowering drugs) might, or might not, have
the same effects.
There was some disagreement among the editors of the Journal as to whether to publish the study,
which challenges the standard school of thought in U.S. cholesterol
management that lower is better. Ideally, a study would give clearer insight as to how doctors and patients should proceed.
However, as the editors pointed out, the findings, though provocative, did not provide clear answers and much more research
must be done to provide doctors and their patients with a recommendation for the appropriate management of cholesterol levels.
The editors chose to publish the article although its practical impact would be unclear, saying: “In the five years
that we have been stewards of the Journal, no other manuscript has stimulated such intense scrutiny and discussion.”
New study builds on existing experience
The authors and editors were very concerned by the study’s finding, especially because
similar evidence has existed for decades.
An increased incidence in side effects has been associated with low cholesterol since as early
as 1971. That year a Japanese report showed a correlation between bleeding in the brain and very low cholesterol levels. This
study was followed in the 1970s and 1980s with a number of other studies showing a surprising increase in mortality from noncardiovascular
causes (cancer, respiratory, digestive, trauma) as cholesterol levels fell. Those findings caused enough worry at the National
Institutes of Health’s National Heart, Lung and Blood Institute (NHLBI) that the agency called a conference to discuss
the matter.
The NHLBI conference, held in 1990, examined data from 20 studies, including those from the U.S.,
Europe, Japan and Scandinavia.
Data were pooled to examine outcomes in men and women as a function of their total cholesterol levels. Some studies were observational
(no drugs involved); others were tests of cholesterol-lowering drugs. One analysis showed that the chance of death due to
cancer, trauma, respiratory and digestive causes was actually increased
at low total cholesterol levels. In fact, the only cause of death that decreased
as cholesterol levels fell was cardiovascular (45 percent of deaths).
Medical community should recognize potential relationship
With the present study being larger than previous ones and therefore more convincing, there needs
to be a more honest acceptance of this “disturbing” potential relationship so that physicians and patients can
make more realistic choices between drug risks and benefits.
What You Can Do
Patients undergoing treatment for cholesterol levels should discuss with their physicians how
low they are aiming to get their cholesterol levels, bringing to the doctor’s attention concerns about the dangers of
very low cholesterols and discussing the differences between the goals for lowering cholesterol for primary and secondary
prevention (see box below).
If cholesterol remains high despite diet,
add 10 grams of psyllium (METAMUCIL, PERDIEM) a day. Numerous studies have shown that psyllium, for example five grams twice a
day, can significantly lower total cholesterol and LDL cholesterol.1 Psyllium, a naturally occurring vegetable fiber,
is clearly safer than any of the cholesterol-lowering drugs.
Levin EG,
Miller VT, Muesing RA, Stoy DB, Balm TK, LaRosa JC. Comparison of psyllium hydrophilic mucilloid and cellulose as adjuncts
to a prudent diet in the treatment of mild to moderate hypercholesterolemia. Archives of Internal Medicine Sep 1990;
150: 1822 - 1827.
Cholesterol-Lowering2 Drugs for People 70 and Older
It is clear that the
relationship between moderately elevated cholesterol levels and increased risk of heart disease is not as clear as people
get older.2 As geriatricians Fran Kaiser and John Morely have written:
Given the uncertainty of the effects of cholesterol manipulation
in older individuals, what should be the approach of the prudent geriatrician to hypercholesterolemia (elevated blood cholesterol
levels)? In persons over 70 years of age, life-long dietary habits are often difficult to change and overzealous dietary manipulation
may lead to failure to eat and subsequent malnutrition. Thus in this group minor dietary manipulations such as the addition
of some oatmeal (or other sources of oat bran or soluble fiber) and beans and modest increases in the amount of fish eaten,
may represent a rational approach. Recommending a modest increase in exercise would also seem appropriate. Beyond this, it
would seem best to remember that the geriatrician’s dictum is to use no drug for which there is not a clear indication.3
The use of cholesterol-lowering drugs in people 70 or older
should be limited to patients with very high cholesterol levels (greater than 300 milligrams) and those who manifest cardiovascular
disease (previous history of heart attack or angina).4
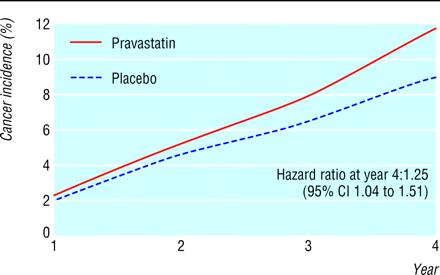
The only large clinical trial looking exclusively at the effect of statins on people over the
age of 70 provides clear evidence for avoiding these drugs for use in primary prevention of cardiovascular disease in older
people who have not had a previous heart attack, stroke, angina, or other cardiovascular diseases or family history. Five
thousand eight hundred and four people aged 70 through 82 were randomized to get a statin or a placebo and were followed for
an average of 3.2 years. For the more than 3,200 people in this study without prior cardiovascular disease, the statin had
no beneficial effect in preventing subsequent cardiovascular disease. There was, however, a significant
25% increased amount of cancer in those getting the statin, particularly gastrointestinal cancers, the cancer predicted in
the animal studies of these drugs (see below). The increase was larger the greater the number of years the drug was being used. No other study analyzing cancer
exclusively in large numbers of older patients getting statins has refuted this finding of increased gastrointestinal cancer.5
In summary, people over 70 using statins for primary prevention
of cardiovascular disease have no benefit, compared to a placebo, but an increased risk of muscle damage (rhabdomyolysis),
liver damage, and, as found in the study described above, an increased risk of cancer. It needs to be emphasized, however,
that for those over 70 who have had previous cardiovascular disease, the use of statins may be beneficial.
There are even questions as to whether elderly people who are hypertensive should have their
cholesterol lowered by drugs. One review concluded, “Further trials are required before routinely suggesting that it
is advantageous to lower cholesterol in an elderly hypertensive who does not have pre-existing evidence of coronary heart
disease.”6
Animal studies consistently show a cancer-causing effect for the
two most popular classes of cholesterol-lowering drugs, the fibrates or fibric acid derivatives, which include clofibrate
(ATROMID-S) and gemfibrozil (LOPID), and the widely used statin drugs, fluvastatin (LESCOL), lovastatin (MEVACOR), pravastatin
(PRAVACHOL), and simvastatin (ZOCOR). Evidence of a cancer-causing effect from these drugs based on clinical trials
in humans is inconclusive because of inconsistent results and a follow-up period that, to date, is
too short to detect some cancers that can take years to develop. The ultimate effect of cholesterol-lowering drugs
in humans may not be known for decades.
Researchers have taken the rodent cancer data from the 1992 and 1994 editions of the Physicians’
Desk Reference (PDR, a compilation of package inserts available in many public libraries).
The package inserts for cholesterol-lowering drugs show that all the fibrates and statins cause cancer in rats and mice. Rats and mice are used because almost all known agents that cause cancer in humans have been found to cause
it in these animals. In most instances, cancer-causing dose levels corresponded to maximums recommended for humans. In a six year study it was found that for those over 70 without previous cardiovascular
disease, there was no benefit but there was an increased risk of cancer, especially gastrointestinal cancer.
Although there is clear evidence that certain of the statin drugs not only lower total cholesterol
and LDL cholesterol (the “bad” cholesterol) but also decrease the risk of heart
attacks and strokes, this evidence is strongest for people who are at much higher risk of these diseases because they have
already had a heart attack, angina, bypass surgery or angioplasty, or a stroke.
The evidence for treatment, especially with cholesterol-lowering drugs, is much weaker for people
who have not yet had the cardiovascular disease described above, known as primary prevention. This is especially so for those
people who do not have more than one of the following risk factors: hypertension, diabetes, smoking, obesity, or a close family
history of premature heart attacks or strokes.
I believe that the lowering
of event in the high-risk group is due to the aspirin like ability to lower thrombi, and not because of the lowering of LDL—jk.